CGRP is an ubiquitous peptide that is not only involved in migraine, but also in several physiological processes and in homeostatic responses during pathophysiological conditions. As such, it is vital to consider the possible side effects caused by the non-selective blockade of α- and β-CGRP with the CGRP (receptor)-antibodies. Even though the knowledge of the presence and function of CGRP in the CNS is sparse, the function in both the peripheral and enteric nervous system is well established and CGRP is expressed widely throughout both systems. Thus, a wide variety of possible adverse events could be anticipated when blocking CGRP. However, reported adverse events after blocking of CGRP have in general been mild to moderate and the incidences have been low.
In the cardiovascular system, CGRP is present in nerve fibers that innervate blood vessels and the heart, and participates in the regulation of blood pressure. Furthermore, it has also been described to have a role in the maintenance of (cardio)vascular homeostasis during ischemic events and in tissue remodeling in pulmonary hypertension. This protective role raises a concern, since migraine patients present an increased cardiovascular risk. Hence, it is important to consider preexisting cardiovascular risk factors in patients (i.e. family history, tobacco exposure, obesity) to prevent a possible cardiovascular event.
Although CGRP participates in inflammatory processes, it has also been associated with facilitation of wound healing. This is thought to be mediated through its ability to promote keratinocytes proliferation, enhance revascularization, reduce expression of tumor necrosis factor-α (TNF-α) and attenuate macrophage infiltration. A consequence of blocking CGRP could thus be alterations in wound healing and increased inflammatory responses in skin injuries at the site of injection for the antibodies. However, this is a theoretical risk which has so far not been observed in clinical trials.
The antibodies against CGRP are not selective for α-CGRP but also block β-CGRP. The gastrointestinal tract is highly innervated by β-CGRPergic fibers from the enteric nervous system. In fact, animal studies with antibodies against CGRP showed extensive mucosal damage, suggesting a role of CGRP in maintaining the mucosal integrity of the gastrointestinal tract. Blocking this could thus contribute to inflammatory bowel disease. Gastrointestinal motility is also considered to be modulated by CGRP, and administration of this peptide induces a dose-dependent biphasic response, which could lead to episodes of diarrhoea or constipation. Furthermore, studies with CGRP KO mice have suggested CGRP agonists as a possible treatment for ulcer healing; therefore, monitoring of gastrointestinal complications (i.e. ulcers, constipation) is recommended, even though 12 week studies have not reported these.
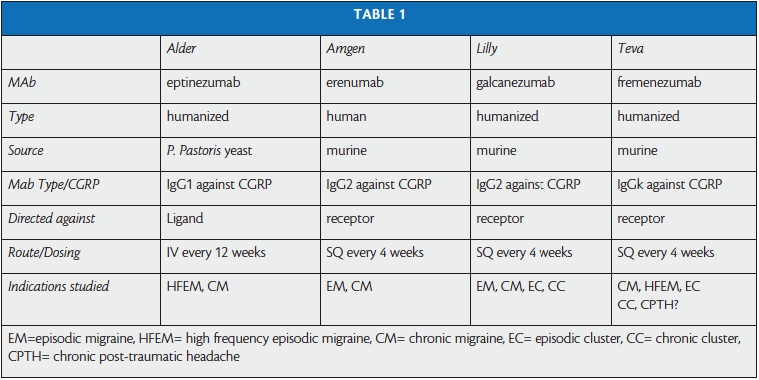
Most importantly, none of the mABs have shown liver toxicity. This is in line with the theoretical probability of mABs causing liver toxicity, which is very low, since metabolism of mABs do not result in production of toxic metabolites. In addition, despite the potentially harmful inhibition of vasodilation due to CGRP inhibition, no cardiovascular concerns have been disclosed with any of these drugs. In trials, eptinezumab, galcanezumab and fremanezumab, monoclonal antibodies which all target CGRP, showed variable percentages of adverse events, which in line with the gepants, were mild to moderate (e.g. upper respiratory or urinary tract infection, fatigue, back pain, arthralgia, nausea and vomiting). Erenumab, which binds to the CGRP receptor, was also safe and well tolerated in a phase 2 trial. No central side effects have been reported.
The long-term risks of blocking CGRP are still unknown. Even though the absence of liver toxicity or other abnormalities in routine blood testing is in support of no or low long-term risks, studies testing the cardiovascular safety of the long-term blockade are warranted in order to answer the numerous questions on the possibility of higher risk in cardio- and cerebrovascular compromised patients. For example, it is unknown whether blocking CGRP could potentially transform transient mild cerebral ischemia into a full-blown brain infarct and whether these risks are higher in women. To investigate these aspects, future studies should include patients with preexisting cardiovascular conditions.
The exact site of action of blocking CGRP is still partly unknown and CGRP could exert its effects on receptors distinct from the CGRP receptor. Recently it was put forward that CGRP may act on the amylin receptor in Trigeminal Ganglion as well as in human coronary arteries. If this is the case, this could pose an additional – unknown – potential risk of wiping out CGRP. We can also only guess whether patients not benefitting from receptor blockade would benefit from blockage of the peptide itself. Future studies should investigate how to differentiate responders from non-responders.
A disadvantage when using antibodies is the risk of development of antibodies against the drug. Indeed, antidrug antibodies were detected with all four antibodies, but these did not seem to affect efficacy. However, long-term studies are needed to investigate whether, at long term, neutralizing antidrug antibodies will pose a problem for efficacy and safety of blocking CGRP with monoclonal antibodies.