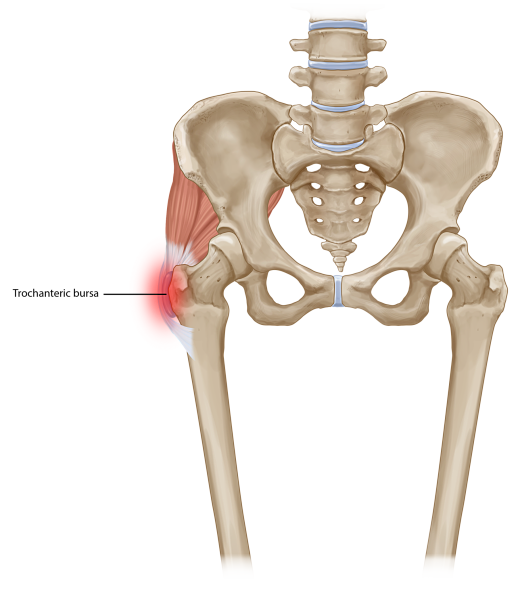
Many risk factors have been associated with GTPS, including age, female gender, ipsilateral ITB pain, knee OA, obesity, and LBP. Because trochanteric bursitis can result from friction between the bursae and greater trochanter, it frequently occurs with overuse or trauma, especially falls. However, misdiagnosis is
common.
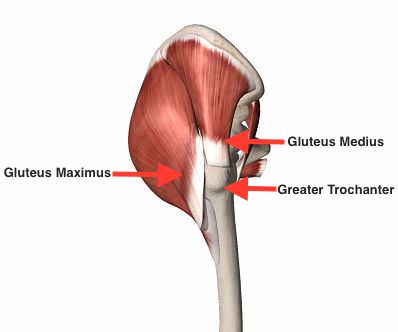
Conditions other than actual bursal inflammation and gluteal tendinopathy that may result in lateral hip pain include gluteus medius muscle dysfunction, ITB syndrome, meralgia paresthetica, OA, and lumbar spine disorders.
Specific etiologies of GTPS include repetitive activity, acute trauma, crystal deposition and infection, especially tuberculosis. When an inciting event can be identified, the initial pathology usually occurs at tendinous attachments to the greater trochanter, with secondary involvement of adjacent bursae. In cases of acute trauma or the presence of other risk factors, extra caution should be exercised so that a more serious condition, such as femoral neck stress fracture or avascular necrosis.