About Pain Spa
We focus on a holistic approach to pain management, encouraging healthy life style changes and promoting overall well-being.
Find out more
About Pain Spa
We focus on a holistic approach to pain management, encouraging healthy life style changes and promoting overall well-being.

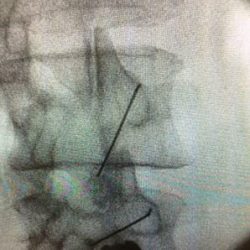 The procedure is usually done on an outpatient basis. The procedure is performed under fluoroscopic guidance to ensure accuracy of needle placement. Patients need to be aware that the outcome of the procedure is variable and they may not receive the desired benefits. Similarly, they must be aware of the transient nature of the therapeutic benefits and that there may need repeated injections.
The procedure is usually done on an outpatient basis. The procedure is performed under fluoroscopic guidance to ensure accuracy of needle placement. Patients need to be aware that the outcome of the procedure is variable and they may not receive the desired benefits. Similarly, they must be aware of the transient nature of the therapeutic benefits and that there may need repeated injections.