Breaking the Myofascial Neck Pain Cycle: The Best Exercises That Actually Work

Best Exercises for Myofascial Neck Pain: A Pain Spa Guide (With Videos)
Myofascial neck pain is one of the most common causes of persistent neck discomfort. It is typically driven by muscle tension, trigger points (“knots”), postural overload, stress-related muscle guarding, and sometimes central pain amplification. The good news is that targeted exercises — performed correctly and consistently — can reduce pain, improve mobility, and help prevent recurrence.
What is myofascial neck pain?
Myofascial pain arises from tight, sensitive areas within muscle known as trigger points. These can cause local tenderness and can also refer pain into the head, jaw, shoulders, or upper back.
Commonly involved muscles include:
- Upper trapezius
- Levator scapulae
- Sternocleidomastoid
- Scalenes
- Cervical paraspinals
- Rhomboids- major & minor (between the shoulder blades; often overloaded with prolonged sitting and rounded shoulders)
Typical contributors include prolonged desk work, sleep position, stress, deconditioning, previous injury/whiplash, and sustained awkward posture.
Why exercise works (and what “good” feels like)
- Improves blood flow and reduces muscle hypertonicity
- Reduces protective guarding and improves movement confidence
- Restores normal neck, shoulder and upper back mechanics (including rhomboid/scapular control)
- Builds postural endurance (so symptoms flare less easily)
- Helps “turn down” pain amplification over time in sensitised systems
Key rule: aim for a gentle pull or mild ache (up to 3/10 discomfort). Avoid sharp pain, electric/radiating pain into the arm, or worsening symptoms for more than 24 hours.
Pain Spa “10–15 minute” home routine
Do this daily for 2–3 weeks, then reduce to 3–4 times per week for maintenance.
1) Warm-up (2 minutes): shoulder rolls, gentle neck turns left/right, chin nods (small range), thoracic extension over a chair back.
2) Self-release (3–5 minutes): use a ball or your fingers to apply steady pressure to tender points (30–60 seconds each), then slowly release.
3) Stretching (3–5 minutes): hold each stretch 20–30 seconds, repeat 2–3 times, stay relaxed.
4) Activation (2–3 minutes): chin tucks + shoulder blade setting (scapular retraction) to recruit mid-back muscles (including rhomboids) and reduce neck overload.
Consistency beats intensity. If you have a flare, shorten the routine and keep movements smaller — don’t stop completely unless advised.
Video 1: Neck & shoulder trigger point exercises (your link)
How to use it: do the self-release section first, then stretching, then finish with gentle activation.
Video 2: Myofascial neck pain exercise routine (mobility + control)
This video focuses on gentle movement, mobility, and control — useful for building a daily baseline routine.
Video 3: Self myofascial release (ball technique)
Self-release can be particularly helpful for the upper trapezius and paraspinal muscles. Apply steady pressure for 30–60 seconds and breathe slowly.
Tip: you should feel “therapeutic discomfort” but not sharp pain. Avoid pressing directly on the front of the neck.
Video 4: Levator scapulae release (common culprit)
The levator scapulae is a frequent driver of one-sided neck stiffness and headache-type pain, especially in desk workers and people who carry tension in the shoulders.
Tip: keep the shoulder down on the side being stretched. Don’t yank the head — slow and steady is best.
Video 5: Quick daily neck pain relief stretches (easy follow-along)
This short routine is useful as a “minimum effective dose” on busy days, and can complement the trigger point work above.
GP / Clinician summary: Myofascial neck pain responds well to graded mobility, self-release, stretching and postural activation (including scapular control and rhomboid recruitment). Persistent cases should prompt assessment for facet-mediated pain, discogenic contribution, radicular symptoms, or central sensitisation. Interventions (e.g., ultrasound-guided trigger point injections or diagnostic blocks) should complement — not replace — rehabilitation.
When to seek medical review urgently
Please seek urgent medical attention if you have:
- New significant arm weakness, numbness, or progressive tingling
- Severe pain after major trauma (e.g., fall/accident)
- Fever, unexplained weight loss, or history of cancer with new severe neck pain
- Balance problems, clumsiness, or changes in walking
- Severe headache unlike your usual pattern, especially with neurological symptoms
Don’t forget the mid-back: why rhomboids matter
If your upper back and shoulder blades are “switched off” (common with prolonged sitting and rounded shoulders), the neck muscles often work overtime. Building gentle endurance in the mid-back can reduce neck load.
Simple rhomboid activation: sit or stand tall, gently draw the shoulder blades back and slightly down (as if tucking them into back pockets), hold 3 seconds, repeat 8–12 times, 1–2 sets.
Common mistake: shrugging upwards (this over-recruits upper trapezius). Keep shoulders relaxed and movement subtle.
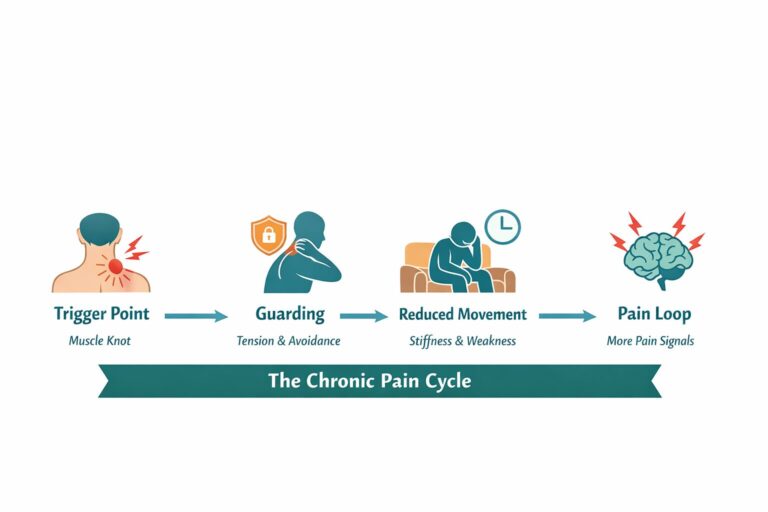
Why symptoms can persist (and why that doesn’t mean “damage”)
Myofascial neck pain often behaves like a sensitised soft-tissue system: muscles become guarded, movement reduces, sleep and stress worsen symptoms, and the nervous system becomes more protective. This does not necessarily indicate structural harm, but it does mean your system may need a graded, consistent plan rather than repeated rest.
If you find that every attempt at exercise causes a flare, reduce intensity, shorten sessions, and build up more slowly — sometimes with physiotherapy guidance.
Frequently Asked Questions
How often should I do these exercises?
Daily for 2–3 weeks is a good starting point, then 3–4 times per week for maintenance.
Should the exercises hurt?
Mild discomfort is acceptable. Sharp pain, radiating arm pain, or prolonged worsening after the routine suggests you should modify the approach or seek clinical advice.
How long before I notice improvement?
Many people notice gradual improvement within 2–4 weeks, especially with daily consistency and improved posture habits. If there is no meaningful change after 4–6 weeks, consider a specialist assessment.
Can scans miss myofascial pain?
Yes. Myofascial pain does not show on MRI or X-ray because it is primarily a functional muscle/fascia condition rather than a structural abnormality visible on imaging.
Do I need a massage or injection for trigger points?
Not always. Many patients improve with self-release and exercise alone. In persistent cases, targeted treatments (e.g., ultrasound-guided trigger point injections) may help improve tolerance to rehabilitation — but they work best alongside a structured exercise plan.
Need a specialist assessment?
If you have persistent neck pain despite consistent exercise, Pain Spa can provide a detailed consultant-led assessment to identify the primary pain driver and tailor treatment accordingly. We may discuss physiotherapy planning, ergonomics, ultrasound-guided injections where appropriate, and strategies to reduce flare-ups and build long-term resilience.
Rehabilitation remains the foundation — but precision diagnosis helps ensure the right treatment at the right time.
To book a consultation, please contact Pain Spa at clinic@painspa.co.uk or visit www.painspa.co.uk for further information.