The basic physical examination should include the following components:
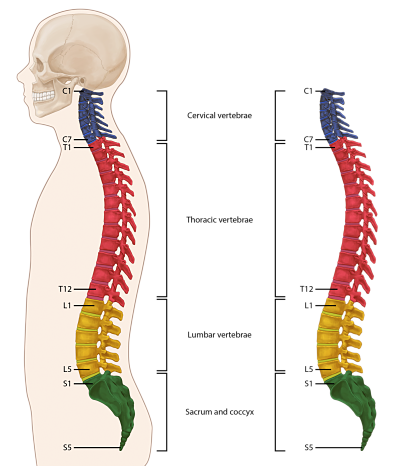
Inspection of back and posture – Inspection of the patient on physical examination can reveal anatomic abnormalities such as scoliosis (lateral spinal curvature) or kyphosis (spinal curvature with posterior convexity).
Range of motion in flexion and extension does not reliably distinguish among pathologic causes, but can provide a baseline to use as an index of therapeutic response. Limited lumbar flexion is not sensitive or specific for diagnosing ankylosing spondylitis.
Palpation of the back is usually performed to assess vertebral or soft tissue tenderness. Vertebral tenderness is a sensitive, but not specific, finding for spinal infection. However, the finding of soft tissue tenderness is poorly reproducible among observers.
The straight leg raise test may be useful to help confirm radiculopathy. Straight leg raising is done with the patient supine. The test is considered positive when the sciatica is reproduced between 10 and 60 degrees of elevation.
The crossed straight leg raising test refers to elevation of the unaffected leg. The test is positive when lifting the unaffected leg reproduces the sciatica in the affected leg. The seated straight leg test is done while the patient is in the seated position and the lower leg is slowly extended until the leg is flexed at the hip to 90 degrees. If sciatica is present, the pain will be reproduced as the leg is extended.
A positive straight leg test has limited sensitivity and specificity for herniated disc (64 and 57% respectively). The crossed straight leg test is less sensitive for herniated disks, but has 90% specificity.
Neurologic assessment of L5 and S1 roots – For patients suspected of having a disc herniation, neurologic testing should focus on the L5 and S1 nerve roots, since 98 percent of clinically important disc herniations occur at L4-5 and L5-S1. Absent reflexes can occur in 30 percent of those between ages 61 and 70 and nearly 50 percent of those aged 81 to 90.
Peripheral pulses – Especially in older patients with exercise-induced calf pain to rule out vascular claudication.
Nonorganic signs or Waddell’s signs – In patients with chronic pain, psychological distress may amplify low back symptoms, and may be associated with anatomically ‘inappropriate’ physical signs. The most reproducible of these signs are superficial tenderness, distracted straight leg raising (ie, discrepancy between seated and supine straight leg raising tests), and the observation of patient overreaction during the physical examination, also known as Waddell’s signs. Other Waddell’s signs suggestive of symptom enhancement include non dermatomal distribution of sensory loss, sudden giving way or jerky movements with motor examination, inconsistency in observed spontaneous activity (dressing, getting off table) and formal motor testing, and pain elicited by axial loading. The presence of multiple Waddell’s signs may suggest a behavioral component to a patient’s pain. However, systematic reviews have not found an association between Waddell’s signs and psychological distress, or claims for disability compensation or litigation.
Imaging has limited utility because most patients with chronic low back pain have nonspecific findings on imaging and asymptomatic patients often have abnormal findings. MRI, which is the preferred imaging modality is only recommended for patients with red flags for serious or rapidly progressive disease or radicular symptoms that do not spontaneously resolve after six weeks.