Neck pain can arise from a variety of causes. Systemic diseases, such as rheumatoid arthritis, spondyloarthritis, polymyalgia rheumatica and bony metastases should be considered in appropriate patients. Degenerative changes are the most common etiology for axial neck pain, as described below.
Cervical discogenic pain
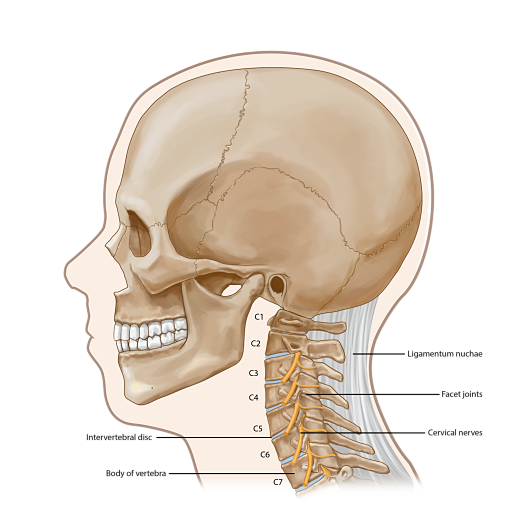
Cervical discogenic pain is probably the most common cause of neck pain. In contrast to patients with cervical disc herniations, cervical discogenic pain refers to derangement in the architecture of the disc that results in mechanical neck pain with or without features of inflammation. The degenerative process that occurs in the intervertebral disc is associated with an inability to effectively distribute pressures between the disc, vertebral endplates, and facet joints.
Axial pain is more severe than extremity pain in cervical discogenic pain. Extremity pain can occur, but is felt to result from somatic referral rather than spinal nerve root impingement. Symptoms are often exacerbated when the neck is held in one position for prolonged periods, such as occurs with driving, reading, or working at a computer. There is often associated muscle tightness and spasms.
Cervical degenerative disc disease is more aptly a radiologic diagnosis, rather than a clinical syndrome, as it is commonly seen on x-ray studies in both symptomatic and asymptomatic patients.
Cervical facet syndrome
The zygapophyseal joint, commonly referred to as the facet joint, can cause axial pain and is probably the most common cause of whiplash-related neck pain and headaches. Pain is often midline or offset slightly to one side. Symptoms can be somatically referred to the shoulders, periscapular region, occiput, or proximal limb. As with cervical discogenic pain, axial symptoms are greater than extremity symptoms.
Unfortunately, there is no specific historical examination, or imaging finding, that provides confirmatory diagnostic information. A fluoroscopically guided injection of local anesthetic to anesthetise the innervation of the joint (cervical medial branch blocks) resulting in pain relief is considered to be the definitive diagnostic test.
Cervical myofascial pain
Regional pain with associated trigger points, taut bands, and pressure sensitivity has been called myofascial pain. Myofascial pain can be a nonspecific manifestation of any pathologic condition that causes pain from the neck to the shoulder and should not be considered a defining diagnosis. Myofascial pain can also be associated with muscle sensitivity, depression, anxiety, insomnia, and may represent a less generalized variant of fibromyalgia.
Diffuse skeletal hyperostosis
Diffuse skeletal hyperostosis (DISH) is a syndrome of inappropriate bone deposition in the insertions of the ligaments and tendons. Large osteophytes connect adjacent vertebral bodies in a somewhat asymmetric fashion. The diagnosis is based on three criteria for spinal radiographs:
• The presence of calcification or ossification along the anterolateral aspects of at least four contiguous vertebral levels.
• Relative preservation of intervertebral disc height in the involved vertebral segments
• The absence of apophyseal joint ankylosis or sacroiliac joint erosions, sclerosis, or intraarticular bony ankylosis.
DISH can be associated with stiffness, loss of mobility, and pain, but can also often be asymptomatic. The bony fusion that results from the hyperostosis may cause mechanical pain at segments adjacent to the fused segments. Prominent anterior vertebral hyperostosis associated with DISH can cause dysphagia.
Cervical radiculopathy
Cervical radiculopathy refers to dysfunction of the spinal nerve root that may manifest with pain, weakness, reflex changes, or sensory changes. Multiple conditions can give rise to cervical radiculopathy, including cervical foraminal stenosis, cervical herniated disc, herpes zoster and diabetic polyradiculopathy, but degenerative changes in the spine are overwhelmingly more common than the other causes, accounting for 70 to 90 percent of cases.