Acromioclavicular osteoarthritis
Acromioclavicular joint pathology is usually well localized. A history of an injury to the joint (shoulder separation), heavy weight lifting, tenderness to palpation at the acromioclavicular joint, pain with cross-body adduction testing, extreme internal rotation, and forward flexion are consistent with the diagnosis. Radiographs may be difficult to interpret because most patients have acromioclavicular osteoarthritis by the age of 40 to 50 years. A distal clavicle lysis or an elevated distal clavicle supports the diagnosis, whereas the absence of tenderness to palpation at the acromioclavicular joint is inconsistent with the diagnosis.
Adhesive capsulitis
Adhesive capsulitis refers to a painful shoulder in which the active and passive ranges of motion are severely limited. Gradual onset of pain and stiffness, loss of motion in all planes with increased pain at the extremes of motion, and a history of diabetes or thyroid disease are consistent with the diagnosis. Radiographs are typically negative, and osteoarthritis on radiography is inconsistent with the diagnosis. A normal range of motion is antithetic to the diagnosis.
Glenohumeral instability
Glenohumeral instability refers to disorders affecting the capsulolabral complex, including dislocation and subluxation. The patients are usually younger than 40 years and have a history of dislocation or subluxation events, which is often involved with collision or overhead sports. A “dead arm,” numbness over the lateral deltoid, and a positive apprehension test are consistent with the diagnosis. Examination findings inconsistent with the diagnosis are no history of dislocation or subluxation and a negative apprehension test. Positive radiographs are helpful for diagnosing Hill-Sachs lesion, dislocation, and inferior glenoid avulsion fracture, but are non-diagnostic if negative.
Glenohumeral osteoarthritis
Glenohumeral osteoarthritis usually presents as gradual pain and loss of motion in patients older than 50 years. A history of arthritis, previous shoulder surgery, pain, crepitus, and decreased motion is consistent with the diagnosis. Radiographs are diagnostic. Normal radiographs and a normal range of motion are inconsistent with the diagnosis.
Rotator cuff pathology
Rotator cuff disorders that affect the function of the rotator cuff include a partial or complete tear, tendinitis or tendinosis, and calcific tendinitis. Initially, it is more important to differentiate this group of disorders from the other groups than it is to identify the specific diagnosis. Typically, the patients are older than 40 years and complain of pain in the lateral aspect of the arm with radiation no farther than the elbow. Weakness, a painful arc of motion, night pain, and a positive impingement sign are components of the history and physical examination that are consistent with this diagnosis. Findings that are inconsistent with this diagnosis include being younger than 30 years, having no weakness, and presenting no impingement signs. Positive radiographs can be helpful to diagnose calcific tendinitis, acromial spur, humeral head cysts, or superior migration of the humeral head, but are typically normal.
Other conditions
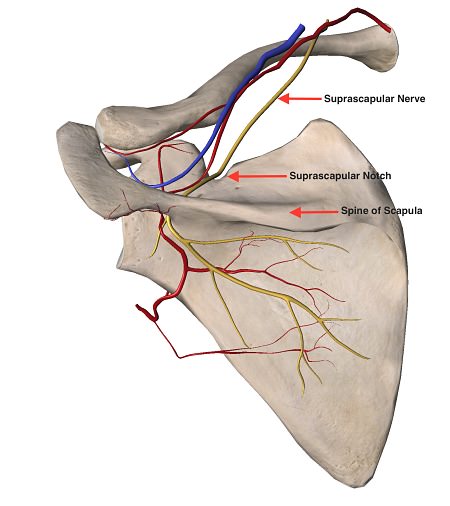
Numerous other problems that can affect the shoulder are somewhat less common, such as biceps and labral pathology (e.g., SLAP tear—superior labrum anterior to posterior tear—an avulsion injury to the root of the long head of the biceps tendon) and multidirectional instability. Other conditions are extremely uncommon, such as a suprascapular nerve injury, Parsonage Turner syndrome (brachial plexus neuritis), and a neuropathic shoulder from syringomyelia. The shoulder can also be the area of perceived pain for many non-shoulder problems, including fibromyalgia, cervical radiculopathy, and thoracic outlet syndrome. Fibromyalgia is notable for classic areas of tender points. Cervical radiculopathy pain is generally posterior, with radiation to the neck and down the arm below the elbow. Thoracic outlet syndrome, like cervical radiculopathy, is notable for symptoms that extend past the elbow and often into the hand. There can be neurologic or vascular symptoms based on the subtype. Positive radiographs are helpful for diagnosing severe cervical osteoarthritis, but are typically negative. Positive provocative shoulder testing (e.g., Hawkins’ impingement test, empty-can test, external rotation test) that disappears after a subacromial lidocaine injection is inconsistent with the diagnosis of fibromyalgia, cervical radiculopathy, or thoracic outlet syndrome.