Persistent Testicular Pain Explained: From Nerve Irritation to Neuromodulation

Testicular Pain and Genitofemoral Neuralgia: When the Pain Is Neuropathic
Chronic testicular pain is one of the most frustrating and distressing pain conditions for patients. It can significantly impair mobility, intimacy, exercise tolerance, and quality of life. Many individuals undergo repeated scans and consultations, only to be told that “everything looks normal.”
When structural causes have been excluded, the next critical step is to consider a neuropathic mechanism.
At Pain Spa Bristol, one of the most important and under-recognised causes of persistent testicular pain is genitofemoral neuralgia.
Understanding why this nerve becomes the pain generator is central to effective treatment.
First and Most Important: Excluding Red Flags
Before diagnosing neuropathic pain, serious and potentially sinister causes must be excluded.
These include:
- Testicular torsion
- Infection (epididymo-orchitis)
- Testicular malignancy
- Inguinal or femoral hernia
- Vascular pathology
- Intra-abdominal or pelvic disease
- Referred spinal pathology
All patients should undergo formal urology assessment and ultrasound imaging of the testes and scrotum. Ultrasound is highly sensitive for torsion, masses, infection, hydrocele, and varicocele.
If symptoms persist and initial investigations are reassuring, further imaging may be clinically indicated:
- CT abdomen and pelvis — to exclude retroperitoneal pathology, lymphadenopathy, occult hernia or post-surgical complications
- MRI pelvis — for deep soft tissue or entrapment pathology
- MRI lumbar spine — when back pain, radicular features, or suspected L1–L2 nerve root irritation are present
Imaging must be symptom-directed and clinically justified. Only when structural causes have been confidently excluded should a neuropathic pain generator be considered.
Understanding the Genitofemoral Nerve
Why This Nerve Can Be the Pain Generator
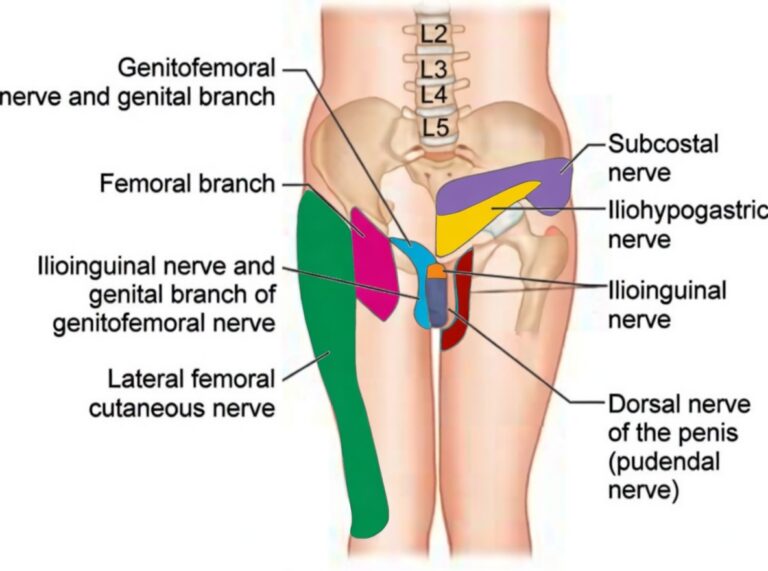
The genitofemoral nerve arises from the L1 and L2 nerve roots of the lumbar plexus. It forms within the psoas muscle and descends anteriorly before dividing into:
- Genital branch — supplying sensation to the scrotum in men (labia majora in women)
- Femoral branch — supplying the upper anterior thigh
When patients describe:
- Burning or electric pain in the scrotum
- Pain radiating into the upper groin
- Hypersensitivity around the pubic tubercle
- Pain worsened by hip extension or walking
the sensory territory often maps precisely onto the genitofemoral nerve.
Why Does the Genitofemoral Nerve Become Painful?
Neuropathic pain can develop due to:
- Post-surgical irritation (hernia repair, pelvic surgery)
- Trauma
- Scar entrapment
- Stretch injury
- Chronic inflammation
- Repetitive mechanical irritation
Over time, the nerve can develop:
- Ectopic discharges
- Sodium channel upregulation
- Hyperexcitability
- Peripheral sensitisation
The nerve begins firing abnormally even in the absence of ongoing tissue damage.
Importantly, because there is overlap with the ilioinguinal and iliohypogastric nerves, selective diagnostic blocks are often required to identify the true pain generator.
Diagnostic Genitofemoral Nerve Block
Once structural causes are excluded and symptoms are consistent with neuropathic pain, an ultrasound-guided genitofemoral nerve block is performed.
This step is critical.
Diagnostic Role
If pain significantly improves following the injection, this confirms that the genitofemoral nerve is the primary pain generator.
This is not guesswork — it is anatomical confirmation.
Therapeutic Role
When combined with local anaesthetic and steroid, relief may last weeks to several months in selected patients.
However, in many cases the benefit is temporary — because the underlying neuropathic firing remains.
This is where escalation becomes necessary.
Pulsed Radiofrequency (PRF) of the Genitofemoral Nerve
If diagnostic block confirms the nerve as the pain generator but relief is incomplete or short-lived, pulsed radiofrequency (PRF) is the next logical step.
This is not a destructive procedure.
It is neuromodulation.
The Neurophysiology Behind PRF
Neuropathic pain involves abnormal electrical activity within the nerve. The genitofemoral nerve may exhibit:
- Persistent ectopic firing
- Abnormal signal amplification
- Reduced firing threshold
- Ongoing spontaneous discharge
PRF applies short bursts of high-frequency electrical energy while maintaining safe, non-destructive temperatures.
This produces:
- Modulation of ion channel behaviour
- Reduction in neuronal hyperexcitability
- Suppression of ectopic discharges
- Dampening of peripheral sensitisation
In simple terms, PRF aims to recalibrate abnormal nerve firing.
The nerve remains structurally intact — but its pathological signalling is reduced.
Why Target the Nerve Peripherally First?
The genitofemoral nerve is the final sensory pathway to the scrotum and groin.
If confirmed as the pain generator, treating it at this precise distal location offers:
- Highly focused treatment
- Minimal risk of widespread sensory change
- Avoidance of unnecessary spinal intervention
- Lower complication profile
This makes peripheral PRF the preferred escalation before considering root-level treatment.
Why Ultrasound Precision Matters
The genitofemoral nerve lies near:
- Femoral vessels
- Inguinal canal structures
- Spermatic cord contents
High-resolution ultrasound allows:
- Real-time visualisation
- Accurate needle positioning
- Avoidance of vascular injury
- Controlled delivery of PRF energy
Technical precision directly influences outcomes.
Dr Krishna’s extensive experience in ultrasound-guided neuromodulation is central to achieving consistent, safe and effective results.
Escalation Strategy: Targeting the Dorsal Root Ganglion (L1–L2)
If response to peripheral PRF is suboptimal or short-lived, the next consideration is the origin of the nerve.
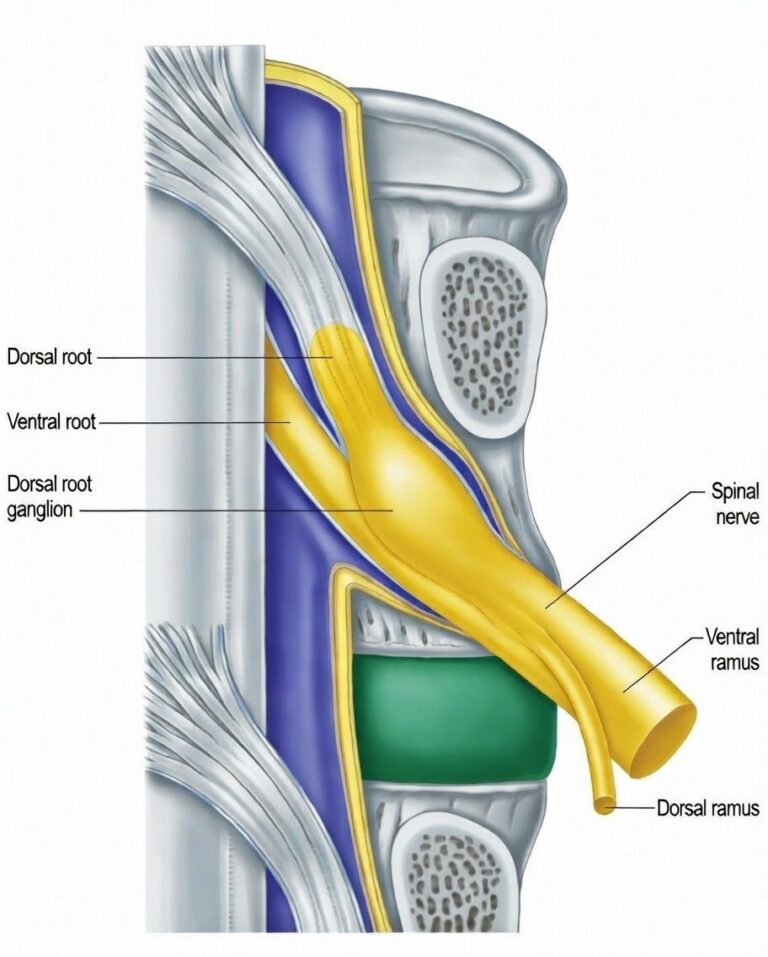
The genitofemoral nerve arises from L1 and L2. The sensory neuron cell bodies reside within the dorsal root ganglion (DRG) at these levels.
Why the DRG Can Sustain Pain
The DRG is a key amplification site in neuropathic pain.
It is where:
- Peripheral signals converge
- Hyperexcitability may be maintained
- Central sensitisation input is generated
- Abnormal discharges can persist
If the pain generator has become root-level rather than purely peripheral, distal treatment alone may not be sufficient.
L1–L2 DRG Block
A fluoroscopy-guided DRG block can confirm proximal involvement.
Significant temporary relief suggests a root-level driver.
PRF of the DRG
If diagnostic DRG block is positive but temporary, PRF of the L1–L2 DRG may be considered.
At this level, PRF modulates the primary sensory neuron cell body itself — potentially producing more sustained dampening of pathological signalling.
This represents a higher-level escalation for carefully selected patients.
Botulinum Toxin for Refractory Cases
In rare cases where pain remains refractory to both peripheral and DRG interventions, botulinum toxin type A may be considered.
Case literature demonstrates meaningful symptom reduction lasting approximately 3–4 months in selected patients.
Structured Escalation at Pain Spa Bristol
Our approach is always stepwise and mechanism-based:
- Exclude red flags and structural pathology
- Confirm neuropathic mechanism
- Ultrasound-guided genitofemoral nerve block
- Pulsed radiofrequency of the genitofemoral nerve (flagship intervention)
- L1–L2 DRG block if needed
- DRG PRF in selected cases
- Botulinum toxin for refractory presentations
This structured escalation avoids unnecessary surgery while providing access to advanced neuromodulation when required.
If you suffer from testicular pain and would like a specialist assessment, please contact Pain Spa at clinic@painspa.co.uk or visit www.painspa.co.uk for further information. A structured, mechanism-based plan can significantly improve outcomes.