Platelet Rich Plasma Therapy Summary
Platelet rich plasma therapy is an innovative treatment that can be used in management of a variety of chronic pain conditions including tendon injuries, muscle injuries and ligament injuries. The potential role of PRP in healing musculoskeletal injuries is an exciting frontier that may lead to newer improved therapies. However, further studies are needed to establish effectiveness, indications and protocols for PRP application in the treatment of musculoskeletal injuries. At Pain Spa Dr Krishna is very experienced in performing interventional pain procedures, including platelet-rich plasma therapy. Dr Krishna always performs injections under ultrasound or fluoroscopy guidance for greater accuracy and improved safety.
At Pain Spa Dr Krishna is very experienced in performing interventional pain procedures, including platelet-rich plasma therapy. Dr Krishna always performs injections under ultrasound or fluoroscopy guidance for greater accuracy and improved safety.

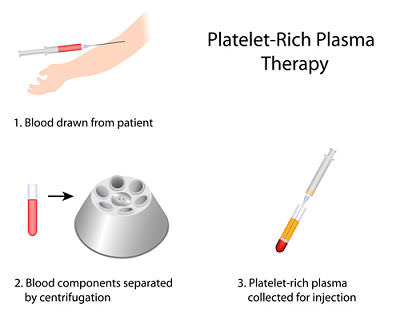 The procedure is usually done on an outpatient basis. Patients need to be aware that the outcome of the procedure is variable and they may not receive the desired benefits. Similarly, they must be aware of the transient nature of the therapeutic benefits and that they may need repeated injections. A series of 3 injections with platelet rich plasma is usually recommended at 4-weekly intervals. The procedure involves the following steps:
The procedure is usually done on an outpatient basis. Patients need to be aware that the outcome of the procedure is variable and they may not receive the desired benefits. Similarly, they must be aware of the transient nature of the therapeutic benefits and that they may need repeated injections. A series of 3 injections with platelet rich plasma is usually recommended at 4-weekly intervals. The procedure involves the following steps: