TMJ Pain and Dysfunction

Headache
Clicking/locking
Neck tension
Bruxism/clenching
TMJ Pain and Dysfunction: Understanding the Myofascial Component
Temporomandibular disorders (often shortened to “TMD”) describe a group of conditions affecting the temporomandibular joint (TMJ), the muscles that move the jaw (the muscles of mastication), and surrounding structures. Symptoms may include jaw or facial pain, ear discomfort, headaches, clicking or popping, locking episodes, restricted mouth opening, and pain that can radiate into the neck and shoulders. While some patients have true joint pathology, a large proportion of TMJ pain is driven primarily by muscular (myofascial) dysfunction rather than structural joint damage.
Key takeaways
- TMJ pain is often driven by the surrounding muscles (myofascial pain) rather than joint damage alone.
- The masseter, temporalis, medial pterygoid, and lateral pterygoid muscles can refer pain into the jaw joint, ear, teeth, and head.
- Neck muscles (especially sternocleidomastoid) and posture commonly amplify TMJ symptoms.
- Treatment works best when matched to the pain driver: muscle overactivity, joint inflammation, degeneration, or instability.
- At Pain Spa, Dr Krishna offers specialist assessment and advanced injection options, including ultrasound-guided deep muscle treatments.
Why the myofascial component matters
Myofascial pain refers to pain arising from muscles and their surrounding fascia. In TMJ disorders, the masticatory muscles can become overloaded (commonly due to clenching, grinding, stress, posture, and compensation for joint irritation), leading to increased tone, fatigue, tenderness, and trigger points. Trigger points can cause local pain and also refer pain into the TMJ region, teeth, ear, temple, forehead, and behind the eye, which is why TMJ pain can mimic dental or ear conditions.
Symptoms and clinical clues
Muscle-dominant TMJ pain often feels like aching, tightness, jaw fatigue, tenderness to touch, and headache that worsens with stress or chewing. Joint-dominant symptoms may include clicking, catching, locking, pain that feels “in the joint,” and reduced opening. Many patients have a mixed picture, which is why assessment of both the joint and muscles is essential before choosing treatment.
Is your pain mainly muscle-related, joint-related, or both?
More suggestive of muscle (myofascial) pain
- Aching/tightness in jaw or face, tender to touch
- Headache/temple pain linked to clenching or stress
- Jaw fatigue with chewing, worse later in the day
- Neck/shoulder tension alongside jaw symptoms
More suggestive of joint-dominant pain
- Clicking/catching/locking or sudden restriction of opening
- Pain felt “in the joint” just in front of the ear
- Worse with wide opening or jaw deviation
- Inflammatory flare pattern (sometimes)
Mixed presentations are common
Many patients have both muscle overactivity and joint irritation. The most effective treatment plans often combine rehabilitation (jaw and neck) with targeted injections based on the dominant driver(s).
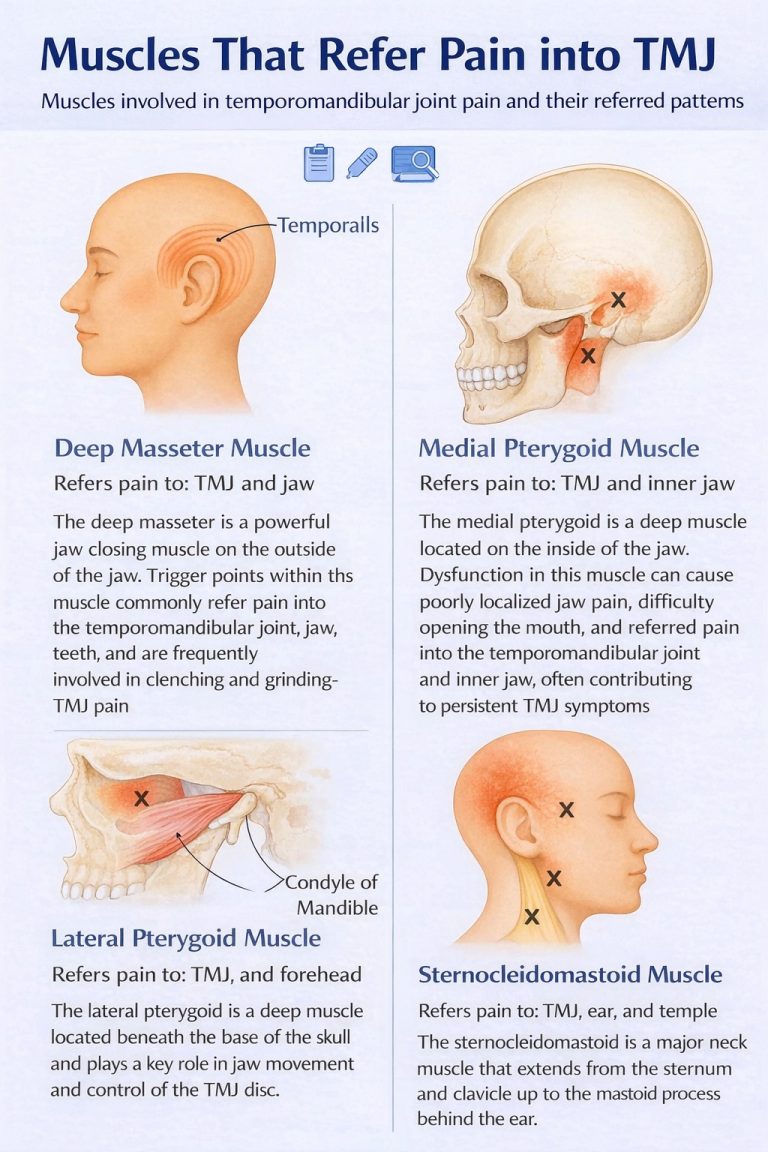
The key muscles that can contribute to TMJ pain
Masseter
The masseter is a powerful jaw-closing muscle at the angle of the jaw and is frequently involved in TMJ pain, especially in people who clench or grind. Overactivity can lead to tenderness, trigger points, and pain referral into the TMJ region, cheek, ear area, and lower teeth, often with jaw tightness and fatigue when chewing.
Temporalis
The temporalis is a fan-shaped muscle at the temples that helps elevate and retrude the jaw. Trigger points here can refer pain into the temple, forehead, and around the eye, and commonly contribute to headache-dominant TMJ presentations, particularly when stress-related clenching is present.
Medial pterygoid
The medial pterygoid is a deep muscle on the inner aspect of the jaw that supports jaw elevation and stability. Because of its depth, dysfunction is sometimes missed. Spasm or trigger points can cause deep, poorly localised pain, jaw tightness, and difficulty opening the mouth, and may perpetuate ongoing symptoms if not addressed.
Lateral pterygoid
The lateral pterygoid is a key muscle for jaw opening, protrusion, and side-to-side movement and plays an important role in controlling TMJ mechanics and the articular disc. Overactivity can contribute to clicking, irritation, locking episodes, and pain that feels “deep in the joint.” Because it is anatomically deep and close to important structures, targeted injection treatment is best performed with advanced anatomical expertise and image guidance.
Muscles around the temporomandibular joint

The neck–jaw connection (including sternocleidomastoid)
TMJ pain frequently coexists with neck and upper shoulder tension. Prolonged desk work, forward head posture, stress, and cervical spine dysfunction can increase the load on the jaw muscles and perpetuate a pain cycle. The sternocleidomastoid (SCM) muscle is particularly relevant because trigger points in the SCM can refer pain into the ear, jaw, temple, and face, sometimes mimicking ear or sinus conditions. Upper trapezius and levator scapulae tension can also contribute via myofascial referral patterns and postural strain, so effective TMJ care often includes addressing both jaw and neck drivers.
Management options for TMJ pain and dysfunction
1) Conservative and self-management measures
Conservative management is the foundation for most TMJ presentations and may include education about jaw “rest posture,” avoiding excessive mouth opening, reducing gum chewing and hard foods, heat therapy, gentle stretching, and pacing jaw activity. Addressing clenching and grinding is crucial. Physiotherapy may include manual therapy, myofascial release, jaw mobility exercises, posture correction, and neck rehabilitation. Dental input (where appropriate) may include occlusal splints or bite guards. Medication options may include simple analgesics and short courses of anti-inflammatory medication when suitable.
2) Trigger point injections (local anaesthetic ± steroid)
For persistent myofascial pain, trigger point injections can be very helpful, especially when discrete tender trigger points are identified on examination. These injections typically involve a small volume of local anaesthetic and, in selected cases, a low-dose corticosteroid. Trigger point injections may be used in the masseter, temporalis, selected deep muscles where clinically appropriate, and contributing neck muscles such as the SCM, as part of a wider rehabilitation plan.
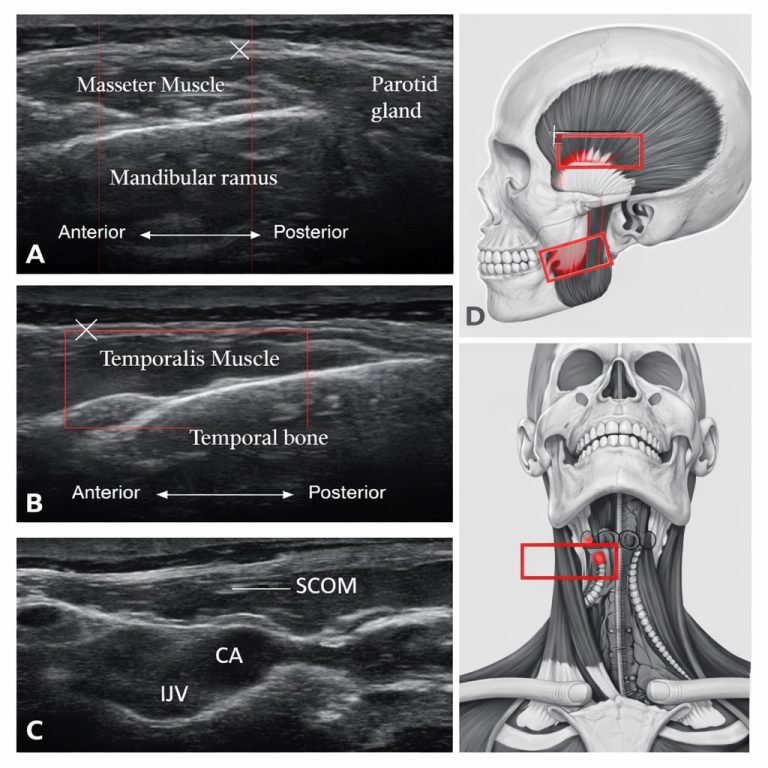
3) Ultrasound-guided TMJ joint injection (local anaesthetic and steroid)
When symptoms are thought to be primarily intra-articular (from within the joint), an ultrasound-guided TMJ joint injection may be appropriate. This involves placing local anaesthetic and corticosteroid into the joint space to reduce pain and inflammation and improve function. Ultrasound guidance improves accuracy and safety by allowing real-time visualisation of the target and nearby structures, and it can also help clarify whether pain is joint-driven or predominantly muscular.
4) Botulinum toxin (Botox) for muscle overactivity
Botulinum toxin (Botox) can be considered when conservative care and trigger point treatments have not provided sufficient relief, particularly in patients with persistent muscle spasm, bruxism-related pain, and overactivity of the muscles of mastication. Botox reduces excessive muscle contraction and can help calm trigger point activity, improving pain and jaw function. Accurate muscle selection matters, and treatment may involve the masseter and temporalis, with consideration of deep muscles such as the medial and lateral pterygoids in selected patients.
5) PRP treatment (platelet-rich plasma)
PRP treatment is a regenerative option used in selected cases, typically when there is suspected degenerative change, early osteoarthritis, or persistent intra-articular symptoms where repeated steroid injections are undesirable. PRP is prepared from the patient’s own blood and contains concentrated growth factors that may help modulate inflammation and support tissue healing. PRP is commonly delivered into the TMJ under ultrasound guidance, and improvement is typically gradual rather than immediate.
6) Prolotherapy (dextrose-based capsular/ligament treatment)
Prolotherapy is an injection-based treatment aimed at selected patients where pain may be driven by capsular or ligamentous laxity and joint instability rather than muscle spasm or active inflammation. It typically involves injecting a solution (most commonly hypertonic dextrose) around specific ligaments or the joint capsule to stimulate a controlled healing response and support connective tissue strengthening over time. In TMJ disorders, prolotherapy may be considered for patients with features such as joint hypermobility, recurrent subluxation, a sense of instability, or pain that worsens with prolonged use due to reduced mechanical support.
Because different injection treatments work in different ways, a clear comparison can help explain why one option may be recommended over another.
Which injection is right for me?
The best option depends on whether your symptoms are mainly driven by muscle overactivity (often Botox or trigger point injections), joint inflammation (often steroid joint injection), degenerative joint irritation (sometimes PRP), or instability/hypermobility (prolotherapy in selected cases).
Steroid vs Botox vs PRP vs Prolotherapy: a clear comparison
Injection treatments for TMJ pain work in different ways and are chosen based on what is driving the symptoms. Some treatments target inflammation within the joint, some reduce overactivity in muscles, and others aim to support longer-term tissue healing or stability. The options below are not “better or worse” than each other; they are designed for different clinical scenarios.
At Pain Spa, treatment selection is guided by a careful assessment of whether symptoms are driven mainly by muscle overactivity, joint inflammation, degenerative change, instability, or a combination. Many patients benefit from a staged approach that combines rehabilitation with precisely targeted injections.
Ultrasound image of muscles around TMJ
TMJ injection expertise at Pain Spa
At Pain Spa, TMJ pain management is led by Dr Krishna, with extensive experience in diagnosing and treating complex facial pain and temporomandibular disorders with a strong focus on the myofascial component. Assessment is anatomy-based and individualised, identifying which muscles and structures are driving pain and dysfunction in each patient.
Dr Krishna has advanced expertise in injection treatments for TMJ pain, including trigger point injections and ultrasound-guided procedures. Ultrasound guidance supports precision and safety, particularly when targeting deep structures.
Dr Krishna is one of a small number of clinicians offering ultrasound-guided lateral pterygoid injection techniques in a specialist setting. Where Botox is appropriate, careful muscle selection and accurate placement are central to achieving good outcomes, particularly for patients whose symptoms are driven by deep muscle overactivity and persistent myofascial pain.
Frequently asked questions
Does TMJ pain always mean there is a problem inside the joint?
Not necessarily. Many patients have muscle-driven (myofascial) pain with a structurally normal joint. Clicking or locking can occur with joint issues, but muscle overactivity and trigger points can also produce significant pain and restricted movement.
How quickly do injections work?
Local anaesthetic can provide immediate short-term relief; steroid may improve symptoms over days. Botox typically takes several days to two weeks to reach full effect. PRP and prolotherapy are usually slower and may build benefit over weeks as part of a structured plan.
Do I still need physiotherapy if I have an injection?
In many cases, yes. Injections can reduce pain and muscle overactivity, but physiotherapy and habit/posture work help address the drivers and improve long-term outcomes.
Can neck tension really cause jaw and ear pain?
Yes. Neck muscles, particularly sternocleidomastoid (SCM), can refer pain into the ear, jaw and temple. Treating both jaw and neck drivers is often important.
Summary
TMJ pain and dysfunction are frequently driven by myofascial dysfunction of the muscles of mastication, including the masseter, temporalis, medial pterygoid, and lateral pterygoid, and symptoms are often influenced by neck muscle tension and posture, including sternocleidomastoid involvement. Management is most effective when tailored to the underlying pain driver and may include conservative measures, physiotherapy, trigger point injections (local anaesthetic ± steroid), ultrasound-guided TMJ joint injection (local anaesthetic and steroid), botulinum toxin (Botox) for overactive muscles, and selected regenerative options such as PRP treatment and prolotherapy.
Ready for an assessment?
If your jaw pain, facial pain, headaches, clicking/locking, or restricted opening is affecting sleep, eating, or daily life, a specialist assessment can clarify whether symptoms are muscle-driven, joint-driven, instability-related, or mixed, and guide the most appropriate treatment pathway.
Contact Pain Spa
Or call to discuss appointment options.
Medical note: This information is intended for general education and does not replace an individual clinical assessment. Treatment suitability varies between patients and depends on diagnosis, medical history, examination findings, and shared decision-making.