Thoracic Outlet Syndrome: A Complex and Often Contested Diagnosis

Thoracic Outlet Syndrome (TOS): why it’s difficult, how we assess it, and when targeted injections can help
Thoracic Outlet Syndrome (TOS) is a complex condition where nerves and/or blood vessels can be intermittently compressed as they travel from the neck into the arm. Symptoms can be variable, overlap with many other diagnoses, and may fluctuate with posture and activity, which is why TOS is often missed, mislabelled, or over-diagnosed. This guide explains the anatomy, typical symptoms, the role (and limitations) of clinical tests and imaging, and how ultrasound-guided diagnostic injections (including Botox in selected cases) can support diagnosis and rehabilitation.
Why TOS is tricky
There is no single “gold standard” test for most neurogenic TOS, symptoms can mimic neck or shoulder problems, and many people can have positional vascular changes without true clinical TOS. The most reliable approach is a careful history, focused examination, assessment of posture and shoulder mechanics, appropriate imaging to exclude other causes, and (in selected patients) diagnostic injections to test whether specific muscles are contributing to compression.
The thoracic outlet: key anatomy in plain English
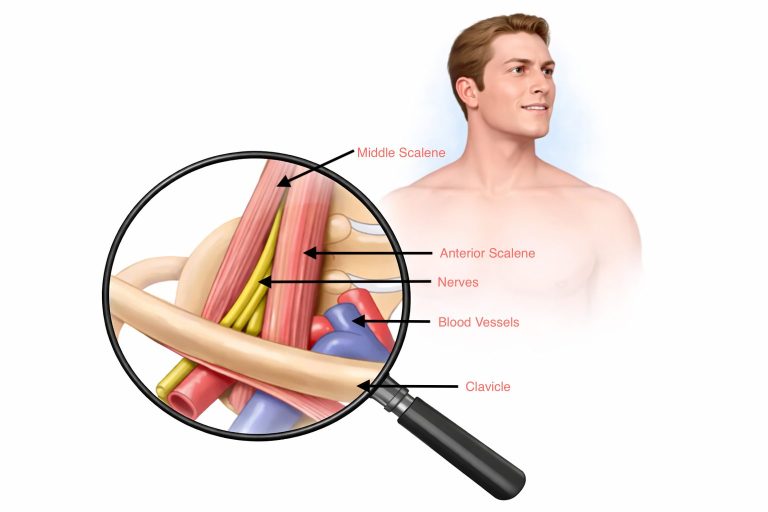
The “thoracic outlet” is not one single tunnel; it is a region where the brachial plexus (nerves to the arm) and the subclavian vessels (artery and vein) pass between the neck, collarbone, first rib, and chest wall on the way into the arm. Compression can occur in more than one place, and it can be positional (worse with lifting the arm, overhead work, or sustained posture).
For patient education, it is usually easiest to think in terms of three common compression spaces:
1) Interscalene triangle (between the anterior and middle scalene muscles): mainly affects the brachial plexus and subclavian artery.
2) Costoclavicular space (between the collarbone and first rib): can affect nerves and blood vessels, particularly with posture (shoulders drooping forward) or load (bags/straps).
3) Subcoracoid / retro-pectoralis minor space (under the pectoralis minor near the coracoid): may contribute to symptoms, especially with shoulder protraction and overhead use.

Types of TOS: neurogenic, venous, arterial
TOS is usually grouped by what is being compressed. Most cases discussed in pain and musculoskeletal clinics are neurogenic (nTOS), but vascular TOS must be recognised because it may require urgent specialist assessment.
Neurogenic TOS (nTOS): symptoms relate to nerve irritation or compression and may include pain, tingling, numbness, heaviness, or fatigue in the arm, often fluctuating with posture or overhead activity.
Venous TOS (vTOS): may present with arm swelling, heaviness, bluish discoloration, and prominent veins; sometimes sudden onset after exertion.
Arterial TOS (aTOS): may cause coldness, pallor, exertional arm pain, and rarely embolic symptoms; it is uncommon but important.
Clinical symptoms and presentation
Symptoms can vary between patients and even within the same patient over time. Neurogenic symptoms commonly worsen with sustained postures (desk work, driving), carrying loads, or overhead activity. Many patients describe a combination of pain and “nerve-like” symptoms rather than a single clear complaint.
Common neurogenic features: neck/shoulder girdle pain, radiating arm pain, tingling or numbness (often ulnar-side but not always), arm heaviness, early fatigue, reduced endurance with overhead activity, and symptoms provoked by posture (rounded shoulders, forward head position).
Features suggesting vascular involvement: swelling, colour change, coldness, prominent veins, or severe exertional symptoms; these should prompt timely vascular assessment.
Examination and clinical tests: what helps (and what doesn’t)
A good examination does more than reproduce symptoms. We assess posture, scapular control, shoulder range of motion, neural tension, distal nerve entrapment signs, and cervical spine features. TOS assessment is often about pattern recognition, not one “positive test.”
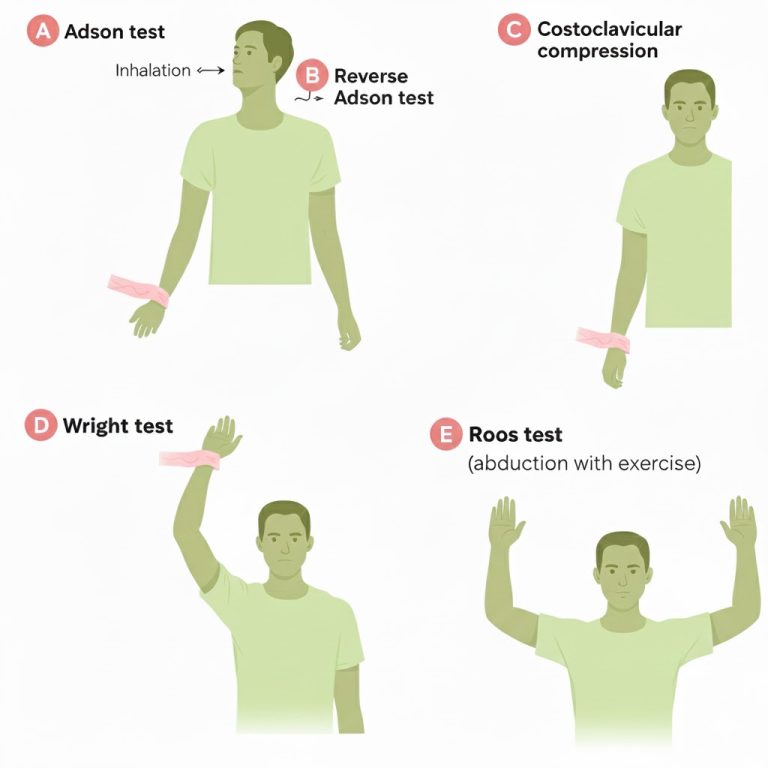
Provocative tests (Adson, Roos/EAST, Wright): why they have limited diagnostic value
Adson test: the patient extends the neck and turns the head toward the tested side (often with a deep breath) while the clinician monitors symptoms and sometimes the radial pulse. A “positive” test is usually taken as symptom reproduction (pulse change alone is not reliable).
Roos test (EAST): the patient abducts the shoulders to 90 degrees, externally rotates, flexes elbows to 90 degrees, then repeatedly opens and closes the hands for up to 1–3 minutes. A “positive” test is typical symptom reproduction (pain, tingling, fatigue, heaviness) rather than simple discomfort.
Wright (hyperabduction) test: the arm is elevated and externally rotated (hyperabducted) while monitoring symptoms and sometimes pulse changes; it may provoke symptoms in those who compress structures under the coracoid/pectoralis minor region.
Why these tests are not definitive: many healthy people can develop pulse changes, numbness, or discomfort with sustained overhead positions; results depend on posture, effort, shoulder mobility, anxiety, and examiner technique. These tests can be supportive when they match the full clinical picture, but they should not “diagnose TOS” in isolation.
Imaging and investigations: useful for exclusion and for vascular TOS, often limited for nTOS
Imaging can be valuable, but it must be interpreted in context. In neurogenic TOS, scans often look “normal,” and that does not rule the condition out. Conversely, anatomical variants can be found in people without symptoms.
Common investigations and what they can (and can’t) do:
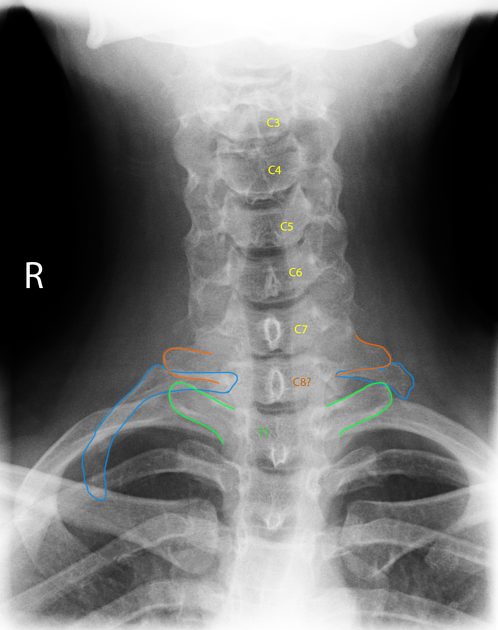
X-ray (neck/chest): can identify bony variants such as cervical ribs or prominent first rib anatomy, and help exclude other bony pathology.
MRI cervical spine / brachial plexus: helpful to assess for alternative diagnoses (disc/foraminal stenosis, tumour, inflammatory disease), but may not show dynamic compression that only occurs in certain positions.
Nerve conduction studies / EMG: useful to assess distal entrapments (carpal tunnel, cubital tunnel) or cervical radiculopathy; many patients with nTOS have normal studies.
Duplex ultrasound (vascular): can assess arterial/venous flow, and can be performed dynamically with provocative arm positioning; it is particularly relevant when vascular symptoms are present.
CT angiography / MR angiography / venography: used mainly for vascular TOS, especially when thrombosis or arterial compromise is suspected; dynamic protocols may be used in specialist centres.
Dynamic investigations: because compression can be positional, tests performed with the arms down may be normal. In selected patients, dynamic ultrasound or positional angiographic studies can demonstrate flow compromise, but abnormal flow alone does not always explain pain symptoms and must be correlated clinically.
Cervical ribs: important clue, not a diagnosis
Cervical ribs (an extra rib arising from the seventh cervical vertebra) can narrow the space for nerves and vessels and may increase the risk of compression, particularly for arterial TOS. However, the presence of a cervical rib does not confirm TOS. Many people with cervical ribs have no symptoms, and many patients with TOS symptoms have no cervical rib. In practice, a cervical rib is best viewed as a “risk factor” or anatomical variant that must be interpreted alongside symptoms, examination, and appropriate vascular assessment if indicated.
Why TOS is misdiagnosed or over-diagnosed
TOS can be mistaken for cervical radiculopathy, shoulder impingement, rotator cuff disease, distal nerve entrapments (carpal tunnel, cubital tunnel), myofascial pain syndromes, or even non-musculoskeletal causes of arm symptoms. On the other hand, because provocative tests are often “positive” in healthy people and imaging can show variants in asymptomatic individuals, some patients are incorrectly labelled with TOS.
A safer approach: confirm that the symptom pattern fits a plausible compression mechanism, ensure red flags and vascular causes are not missed, evaluate for more common conditions first, and use rehabilitation principles (posture, scapular control, graded exposure) before escalating to invasive treatments.
Why pectoralis major is not usually implicated (and pectoralis minor is)
The structures implicated in TOS pass under the collarbone, over the first rib, between the scalene muscles, and (more distally) beneath the pectoralis minor near the coracoid process. The pectoralis major sits more superficially and anteriorly across the chest and does not form the tight anatomical “tunnel” where the brachial plexus and subclavian vessels are typically constrained. For this reason, pectoralis major is not considered a common compressive culprit in TOS, whereas pectoralis minor (due to its position relative to the neurovascular bundle as it enters the arm) can be relevant in selected patients, particularly with rounded shoulders and shoulder protraction.
Diagnostic injections: how they help and which muscles are targeted
Because neurogenic TOS is often dynamic and multifactorial, a targeted injection can act as a functional test. If symptoms improve significantly after anaesthetising (or reducing tone in) a suspected compressive muscle, it supports the idea that this structure is contributing to symptoms. Injections are not a stand-alone diagnosis; they are one piece of a broader assessment.
Common diagnostic targets:
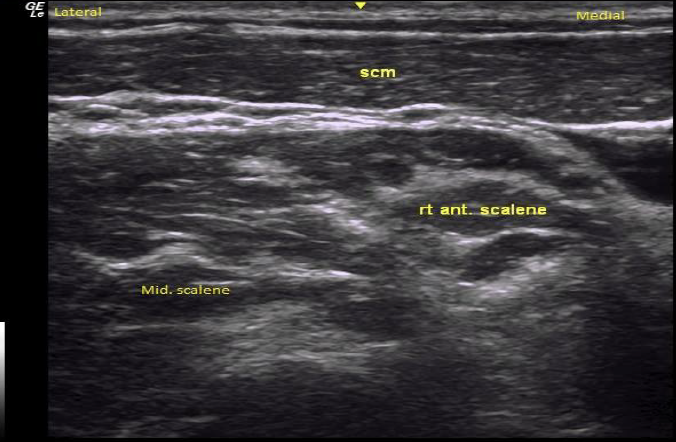
Anterior scalene injection (local anaesthetic ± steroid): Often used when symptoms suggest scalene triangle involvement. Reduction in typical symptoms (even temporarily) can support a working diagnosis and help identify patients who may respond to scalene-focused rehabilitation. This is typically performed with ultrasound guidance to improve precision and safety. This can reduce scalene-related compression/irritation in the interscalene triangle and may improve pain/paresthesia provoked by overhead activity or neck/shoulder posture.
Middle scalene injection: Considered when the clinical picture suggests deeper scalene contribution or when anterior scalene injection alone does not reproduce the expected diagnostic response. The middle scalene sits close to elements of the brachial plexus and can contribute to tethering or irritation.
Pectoralis minor injection: Useful when symptoms are strongly posture-related (rounded shoulders, prolonged desk work) or triggered by overhead position, and when examination suggests tenderness or tightness in the coracoid/pectoralis minor region. This is sometimes described as “pectoralis minor syndrome,” which can mimic or overlap with TOS.
Selected interface injections: in certain cases, targeted local anaesthetic at the costoclavicular interface or adjacent myofascial contributors can help refine the rehabilitation focus, but these must be carefully chosen and are not routine.
Local anaesthetic ± steroid: Local anaesthetic can act as a diagnostic “probe.” Steroid may help if local inflammation is contributing, but the goal is usually diagnostic and rehabilitative rather than long-term suppression.
Botulinum toxin (Botox): Botox may reduce muscle overactivity and spasm for a longer period, creating a window for posture correction and physiotherapy. It is not a cure, but it can be helpful as part of a structured plan in selected patients.
What we look for after a diagnostic injection: meaningful symptom reduction during the patient’s typical provoking activity (e.g., overhead reach, prolonged desk posture), improved endurance, and clearer differentiation from distal entrapment or cervical spine pain.

Botox for TOS: when it may help
Botulinum toxin (Botox) is sometimes used to reduce overactivity or spasm in muscles that may contribute to compression (most commonly the scalenes, and in selected cases pectoralis minor). The aim is not simply pain relief; it is often to create a “rehabilitation window” where reduced muscle tone makes posture work, scapular control, breathing mechanics, and graded strengthening more achievable.
Important limitations: response is variable, benefit may be temporary, and Botox does not “fix” bony constraints or all causes of symptoms. It is best considered when a patient’s presentation strongly suggests muscular contribution and when a structured rehabilitation plan is in place.
Surgery: not straightforward, and not always the best first step
Surgical pathways for TOS (such as first-rib resection and scalenectomy) can be effective in carefully selected patients, especially with confirmed vascular TOS or clearly defined structural compression. However, outcomes are not uniform, complications can occur, and surgery is not a guaranteed solution for complex pain presentations. For neurogenic TOS in particular, non-operative care (rehabilitation, posture and scapular control, activity modification, and targeted injections when appropriate) is usually preferred before considering surgery.
Expertise at Pain Spa
At Pain Spa, Dr Krishna has extensive experience in ultrasound-guided procedures for complex pain conditions. In suspected neurogenic TOS, ultrasound allows precise identification of key anatomy (including the scalene muscles, nearby nerves and vessels) and supports carefully targeted diagnostic injections. This can help confirm whether scalene or pectoralis minor contributions are likely, guide rehabilitation priorities, and reduce unnecessary escalation to invasive pathways.
Ultrasound-guided scalene Botox: in selected patients, Botox into the relevant scalene muscles can reduce muscle tone and spasm, potentially improving symptoms and enabling a more effective physiotherapy programme focused on breathing mechanics, posture, scapular control, and graded strengthening.
What matters most: the injection is only one part of care; the best results are typically achieved when injection findings are integrated into a personalised rehabilitation plan and when alternative diagnoses have been thoughtfully assessed.
Summary: a practical approach
TOS is best approached as a clinical pattern rather than a single test result. We focus on the patient’s symptom behaviour, posture and shoulder mechanics, exclusion of more common conditions, and selective use of imaging and dynamic vascular tests where appropriate. Provocative tests can support suspicion but have poor specificity on their own. Diagnostic injections (local anaesthetic ± steroid, and in selected cases Botox) can provide functional confirmation of muscular contribution and help guide a safer, more effective rehabilitation-first plan.
Need an assessment?
If you have persistent arm symptoms, neck/shoulder pain, or suspected TOS, we can provide a structured assessment and discuss the role of physiotherapy, dynamic investigations (where appropriate), and ultrasound-guided diagnostic injections. Please contact Pain Spa at clinic@painspa.co.uk or via our website www.painspa.co.uk.