Visceral Hypersensitivity: Understanding Chronic Gut and Pelvic Pain Through the Nervous System

Pain Spa | Dr M. Krishna | Specialist Interventional Pain Management
Visceral Hypersensitivity: Why Normal Internal Sensations Can Become Painful
Visceral hypersensitivity, also known as visceral sensitisation, is an important mechanism in many chronic abdominal and pelvic pain conditions. It means that the nervous system becomes unusually sensitive to signals coming from internal organs, so that normal physiological events such as eating, bowel movement, bladder filling or menstruation may be felt as pain, pressure, bloating, urgency or deep discomfort.
This article explains the science behind visceral hypersensitivity, how it differs from abdominal wall pain, how it overlaps with central sensitisation, and how a careful, stepwise treatment plan can help patients with complex abdominal, pelvic and gut-related pain syndromes.
Important note: Persistent abdominal or pelvic pain should always be assessed properly. Visceral hypersensitivity is not a diagnosis of “nothing is wrong”; it is a recognised pain-processing disorder that should only be considered after appropriate assessment for structural, inflammatory, infective, gynaecological, urological, gastrointestinal and abdominal wall causes.
Introduction to Visceral Hypersensitivity
What Is Visceral Hypersensitivity?
Visceral hypersensitivity refers to an enhanced perception of signals arising from the internal organs. In simple terms, the gut, bladder, uterus, pancreas or pelvic organs may send signals that would normally be harmless or only mildly uncomfortable, but the nervous system interprets them as painful, threatening or overwhelming.
This mechanism is well recognised in disorders of gut–brain interaction, particularly irritable bowel syndrome, but it is not limited to IBS. It can also contribute to chronic abdominal and pelvic pain associated with endometriosis, diverticular disease, inflammatory bowel disease in remission, chronic pancreatitis, bladder pain syndrome, chronic pelvic pain syndrome and other overlapping pain conditions.
A key feature is a mismatch between the severity of pain and the visible structural abnormality. Some patients may have severe symptoms despite normal investigations, while others may continue to experience pain after the original inflammation, infection or injury has settled. This does not mean the pain is imagined. It means the pain system has become sensitised.
Visceral Sensitisation vs Central Sensitisation
Visceral sensitisation can start at the level of the organ itself. Nerve endings within the gut or pelvis become more excitable, so normal stretching, pressure, chemical changes or inflammation can trigger exaggerated pain signals. This is called peripheral sensitisation.
Important biological drivers include transient receptor potential channels such as TRPV1, TRPA1 and TRPV4, which are involved in sensing mechanical, thermal and chemical stimuli. These channels can become more active when exposed to inflammatory mediators released by mast cells, immune cells and epithelial cells. Increased gut permeability, low-grade mucosal inflammation and mast cell activity close to enteric nerves can all amplify pain signalling.
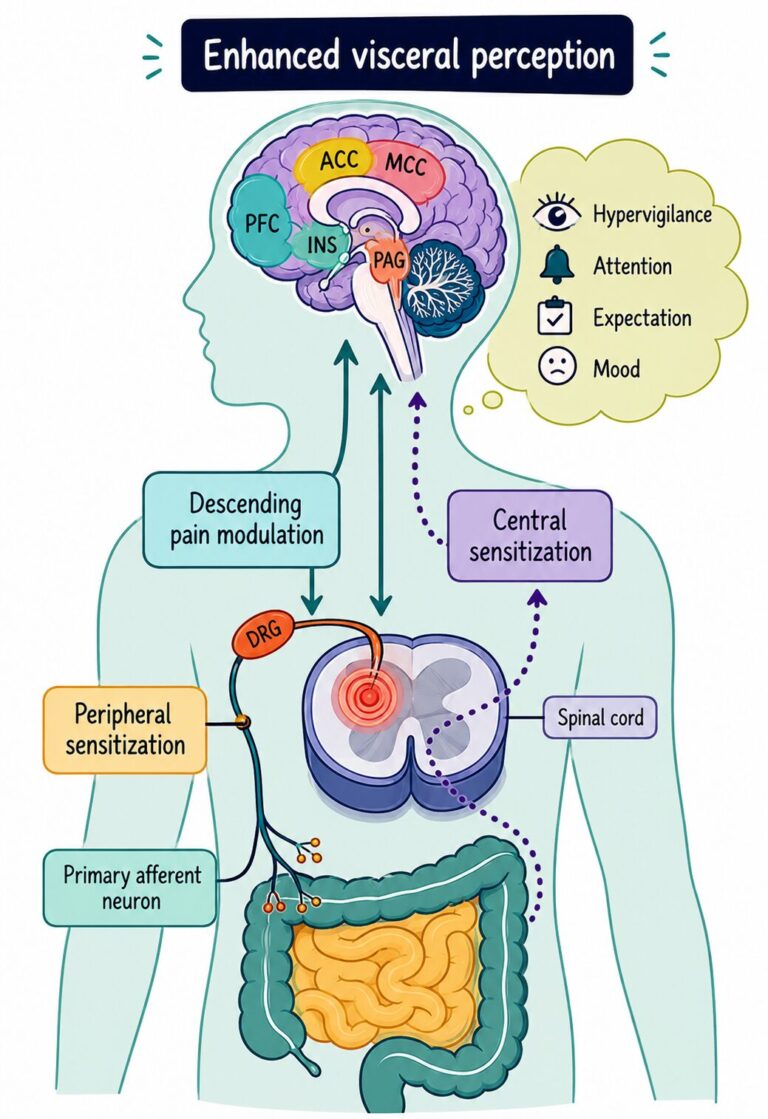
Over time, repeated input from sensitised internal organs can also change how the spinal cord and brain process pain. This is central sensitisation. The spinal cord dorsal horn and brain regions such as the insula, anterior cingulate cortex, prefrontal cortex and hypothalamic stress pathways may become more reactive. The result is that pain becomes easier to trigger, harder to switch off and more likely to spread beyond the original organ.
Practical distinction
Visceral sensitisation means the internal organ-related pain pathways have become more sensitive.
Central sensitisation means the wider nervous system has become amplified, often producing widespread pain, fatigue, sleep disturbance, brain fog, mood symptoms and sensitivity to light, sound, temperature or touch.
Why Normal Internal Sensations Become Painful
Internal organs constantly send information to the nervous system. Normally, most of these signals remain below conscious awareness. We may feel fullness after eating, the urge to open the bowels, bladder filling or menstrual cramping, but these sensations are usually proportionate and temporary.
In visceral hypersensitivity, the threshold for feeling these signals is lowered. Normal gut distension after a meal may be experienced as painful bloating. A normal bowel movement may trigger cramping and urgency. Bladder filling may feel painful earlier than expected. Menstruation may amplify bowel, bladder or pelvic pain because pelvic organs share overlapping nerve pathways.
This can happen after infection, inflammation, surgery, repeated painful episodes, endometriosis, pancreatitis, inflammatory bowel disease, pelvic floor dysfunction, early life stress, psychological stress or prolonged activation of the body’s threat system. The immune system, autonomic nervous system, endocrine system and pain pathways can all become involved.
The Brain–Gut Axis Explained
The brain and gut communicate continuously through the nervous system, immune system, hormones, microbiome and autonomic pathways. This is known as the brain–gut axis. It is not a one-way system. Stress and hypervigilance can increase gut sensitivity, while ongoing gut or pelvic pain can increase stress-system activation, anxiety, poor sleep and central pain amplification.
The hypothalamic–pituitary–adrenal axis, corticotropin-releasing hormone pathways, serotonin signalling, mast cell activation and gut microbiome changes can all influence how visceral pain is processed. This is why visceral hypersensitivity is best understood as a biological pain-processing disorder rather than a purely structural or purely psychological condition.
Effective treatment therefore needs to address both sides of the system: the peripheral drivers from the gut, pelvis or abdominal wall, and the central amplification within the spinal cord, brain and autonomic nervous system.
The Science Behind Visceral Hypersensitivity
Visceral hypersensitivity develops when pain-signalling pathways from internal organs become overactive. This can happen at several levels: within the organ itself, within the nerves carrying signals to the spinal cord, within the spinal cord, and within brain regions involved in pain, threat, emotion, attention and autonomic regulation.
The process is not simply “gut pain” or “stress-related pain”. It is a biological sensitisation process involving nerves, immune cells, mast cells, inflammatory mediators, the gut microbiome, the autonomic nervous system and the brain–gut axis.
Peripheral Sensitisation
Peripheral sensitisation occurs when nerve endings within the gut, bladder, uterus, pancreas or pelvic organs become unusually excitable. These nerves are designed to detect stretch, pressure, chemical irritation, inflammation and tissue injury. In a sensitised state, they begin to fire more easily and send stronger pain signals to the spinal cord.
This can follow inflammation, infection, endometriosis, diverticulitis, inflammatory bowel disease, pancreatitis, pelvic surgery, repeated painful visceral events or persistent immune activation. Even after the original trigger has improved, the peripheral nerves may remain “primed”, so normal physiological activity is perceived as painful.
Central Sensitisation and Nociplastic Pain
If strong visceral pain signals continue for long enough, the spinal cord and brain may become sensitised. This is called central sensitisation. The dorsal horn of the spinal cord becomes more responsive, descending pain-control systems may become less effective, and brain regions involved in pain perception, attention, emotion and threat detection may become more active.
When this process becomes established, pain can become partly independent of the original tissue problem. This is one reason why symptoms may persist even after inflammation has settled, scans appear reassuring, endometriosis has been treated, diverticulitis has resolved, or bowel inflammation is in remission.
This wider pain-processing change is often described as nociplastic pain. It may be associated with widespread pain, abdominal allodynia, fatigue, poor sleep, brain fog, mood disturbance, sensory sensitivity and overlapping conditions such as fibromyalgia, migraine, temporomandibular disorder and chronic pelvic pain.
TRP Channels and Pain Signalling
A key part of peripheral visceral sensitisation involves transient receptor potential channels, often abbreviated to TRP channels. These include TRPV1, TRPA1 and TRPV4. They act like biological sensors on pain nerves and respond to mechanical stretch, heat, chemical irritation, acidity and inflammatory signals.
When TRP channels become upregulated or overactive, the threshold for pain falls. A degree of gut distension, bowel movement, bladder filling or pelvic organ activity that would normally be tolerated may now produce pain, urgency, cramping or deep discomfort.
Mast Cells, Histamine and Neuroinflammation
Mast cells are immune cells that sit close to nerves in the gut and pelvic tissues. When activated, they can release histamine, cytokines, proteases and other inflammatory mediators. These chemicals can irritate nearby sensory nerves and lower the threshold for pain signalling.
This mast cell–nerve interaction is one reason why some patients experience food-related pain, bloating, urgency or visceral discomfort, even when standard tests do not show active inflammation. It may also help explain persistent symptoms in some patients with previous gut inflammation, inflammatory bowel disease in remission, endometriosis or post-infectious gut syndromes.
Histamine pathways are particularly relevant because histamine can increase nerve excitability and contribute to visceral pain. This is why mast cell stabilisers and antihistamine-based approaches are being studied in selected visceral pain states, although these treatments need careful patient selection and should not be presented as a universal solution.
Microglia and Neuroimmune Activation
Microglia are immune-like cells within the central nervous system. When activated, they can release pro-inflammatory signalling molecules that increase the excitability of pain pathways in the spinal cord and brain.
Research suggests that neuroimmune activation in areas such as the spinal cord, hypothalamus and hippocampus may contribute to persistent visceral hypersensitivity. This provides a biological explanation for why chronic visceral pain can become self-sustaining and why treatments aimed only at the original organ may not fully resolve the pain once central sensitisation has developed.
The Role of Serotonin and CRH
Serotonin is an important signalling molecule in the gut as well as the brain. It influences gut motility, secretion and sensory signalling. Altered serotonin signalling, particularly through receptors such as 5-HT3, can contribute to pain, urgency, altered bowel habit and heightened visceral perception.
Corticotropin-releasing hormone, or CRH, is central to the body’s stress response. CRH and CRF1 receptor pathways can increase gut sensitivity, alter bowel function, activate immune pathways and amplify the brain–gut stress loop. This helps explain why stress does not “cause imaginary pain”, but can biologically increase visceral pain sensitivity in susceptible patients.
Gut Microbiome and Neuroimmune Interactions
The gut microbiome communicates with the nervous system through immune mediators, microbial metabolites, gut barrier function, vagal pathways and neuroactive compounds. Changes in the microbiome may influence visceral sensitivity by altering inflammation, intestinal permeability, mast cell activity and gut–brain signalling.
Diet, infection, antibiotics, inflammation and stress can all influence the microbiome. In some patients, changes in microbial signalling may help maintain bloating, urgency, abdominal discomfort and heightened visceral sensitivity. This is one reason why dietary strategies and microbiome-focused treatments may help selected patients, although they should be integrated into a broader pain-management plan rather than used in isolation.
Stress, Trauma and the HPA Axis
The hypothalamic–pituitary–adrenal axis, known as the HPA axis, is one of the body’s main stress-regulation systems. Early life adversity, trauma, chronic stress, anxiety, hypervigilance and prolonged threat activation can all alter how the brain and body regulate pain, immunity, gut function and autonomic tone.
This does not mean the pain is psychological. It means the nervous system, endocrine system and immune system are closely connected. In visceral hypersensitivity, emotional stress and biological pain amplification can reinforce one another through the brain–gut axis.
How Visceral Hypersensitivity Develops
Key Message
Visceral hypersensitivity is best understood as a neuroimmune brain–gut pain-processing disorder. It may begin with inflammation or injury in an internal organ, but over time it can involve peripheral nerves, spinal cord amplification, brain–gut dysregulation, autonomic activation and central sensitisation.
Conditions Associated with Visceral Hypersensitivity
Visceral hypersensitivity is not limited to irritable bowel syndrome. It is increasingly recognised as a shared pain-processing mechanism across multiple gastrointestinal, pelvic and systemic conditions. The common theme is that persistent nociceptive input from inflamed, injured or repeatedly irritated internal organs can sensitise peripheral nerves and alter central pain processing.
Over time, pain may become amplified beyond what would be expected from the original structural abnormality alone. This helps explain why some patients continue to experience severe symptoms despite reassuring scans, disease remission or technically successful treatment of the underlying condition.
Irritable Bowel Syndrome (IBS)
IBS is the classic visceral hypersensitivity disorder. Many patients demonstrate reduced pain thresholds to bowel distension, altered brain–gut signalling and abnormal sensory processing. Normal digestive activity may therefore be experienced as bloating, cramping, urgency or abdominal pain.
Peripheral sensitisation, mast cell activation, altered serotonin signalling, microbiome changes and central sensitisation may all contribute. Stress, hypervigilance and autonomic dysregulation can further amplify symptoms through the brain–gut axis.
Endometriosis
Visceral hypersensitivity is extremely common in endometriosis and helps explain the well-known mismatch between lesion severity and pain intensity. Some patients with relatively limited visible disease experience severe pelvic pain, bowel symptoms, bladder pain, fatigue and widespread sensitisation.
Pain in endometriosis may involve overlapping nociceptive, neuropathic and nociplastic mechanisms. Repeated inflammation, nerve fibre sensitisation, mast cell activation and glial activation can drive persistent peripheral and central sensitisation.
Chronic Pelvic Pain Syndrome
Many patients with chronic pelvic pain develop a broader sensitisation state involving pelvic organs, pelvic floor muscles and the central nervous system. Pain may become disproportionate to visible pathology and may spread between the bowel, bladder, pelvic floor and reproductive organs.
Cross-organ sensitisation and pelvic floor hypertonicity are common. Fatigue, sleep disturbance, widespread pain and autonomic symptoms may indicate progression towards central sensitisation.
Diverticular Disease
Some patients continue to experience abdominal pain long after acute diverticulitis has resolved. Current evidence suggests that low-grade inflammation, neuroimmune activation and visceral hypersensitivity may contribute to these persistent symptoms.
Research has demonstrated increased sensitivity to rectosigmoid distension in symptomatic diverticular disease, suggesting a wider visceral hyperperception state rather than simply local structural irritation.
Inflammatory Bowel Disease in Remission
Patients with Crohn’s disease or ulcerative colitis may continue to experience abdominal pain, urgency and bloating even when inflammatory markers, endoscopy or imaging suggest remission. This does not necessarily mean the disease is “active again”.
Persistent low-grade inflammation, altered pain modulation, mast cell sensitisation and central sensitisation may all contribute to ongoing symptoms despite mucosal healing.
Chronic Pancreatitis
Pain severity in chronic pancreatitis often correlates poorly with imaging findings. Long-standing pancreatic inflammation can lead to nerve sprouting, neural hypertrophy, immune activation and progressive central sensitisation.
Over time, patients may develop widespread hyperalgesia and impaired descending pain inhibition, making the pain increasingly resistant to purely pancreas-directed interventions.
Bladder Pain Syndrome / Interstitial Cystitis
Bladder pain syndrome is closely linked to visceral hypersensitivity and pelvic cross-sensitisation. Patients frequently experience bladder pain, urgency, pelvic pressure and pain with bladder filling despite the absence of obvious infection.
Overlap with IBS, endometriosis and chronic pelvic pain is common because pelvic organs share converging neural pathways within the spinal cord and dorsal root ganglia.
Functional Dyspepsia
Functional dyspepsia involves abnormal sensitivity of the upper gastrointestinal tract. Normal gastric distension after meals may trigger pain, fullness, nausea, bloating or early satiety.
Altered vagal signalling, impaired gastric accommodation, visceral hypersensitivity and central amplification are believed to contribute.
Post-Infectious GI Syndromes
Some patients develop persistent abdominal symptoms after gastroenteritis or other infections. Even after the infection resolves, the nervous system and immune system may remain sensitised.
Persistent mast cell activation, altered microbiome signalling, increased intestinal permeability and low-grade inflammation may help maintain visceral hypersensitivity in these patients.
Long COVID and Visceral Sensitisation
Long COVID is increasingly recognised as a condition involving autonomic dysregulation, neuroimmune activation and central sensitisation. Some patients develop abdominal pain, bloating, altered bowel habit, nausea and visceral sensitivity following COVID infection.
Autonomic dysfunction, mast cell activation, microglial activation and persistent inflammatory signalling may contribute to these symptoms in susceptible individuals.
Fibromyalgia and Overlapping Pain Syndromes
Visceral hypersensitivity frequently overlaps with fibromyalgia, chronic fatigue syndrome, migraine, temporomandibular disorder and chronic pelvic pain. These conditions appear to share abnormalities in central pain processing and sensory amplification.
The presence of multiple overlapping pain syndromes strongly suggests that central sensitisation and altered nervous system regulation are contributing to the patient’s symptoms.
Although these conditions differ structurally, many share common mechanisms involving peripheral sensitisation, neuroimmune activation and central pain amplification.
| Condition | Key Mechanisms | Typical Features | Central Sensitisation Overlap |
|---|---|---|---|
| IBS | Brain–gut dysregulation, mast cells, TRP channels, altered serotonin signalling | Bloating, cramping, urgency, altered bowel habit | Very common |
| Endometriosis | Inflammation, nerve sensitisation, glial activation | Pelvic pain, bowel symptoms, bladder symptoms, fatigue | Very common |
| IBD in remission | Persistent low-grade inflammation, altered pain modulation | Pain despite remission, bloating, urgency | Common |
| Chronic pancreatitis | Neuroplasticity, neural hypertrophy, central amplification | Persistent severe abdominal pain | Common |
| Bladder pain syndrome | Pelvic cross-sensitisation, autonomic dysregulation | Bladder pain, urgency, pelvic discomfort | Very common |
| Functional dyspepsia | Upper GI hypersensitivity, altered vagal signalling | Early satiety, nausea, upper abdominal discomfort | Common |
| Long COVID | Autonomic dysfunction, neuroimmune activation | GI symptoms, fatigue, brain fog | Very common |
| Fibromyalgia | Central pain amplification, altered sensory processing | Widespread pain, fatigue, sensory sensitivity | Core mechanism |
Cross-Organ Sensitisation and Pelvic Cross-Talk
One of the most important concepts in chronic abdominal and pelvic pain is that organs do not function in isolation. The bowel, bladder, uterus, pelvic floor and lower abdominal structures share overlapping nerve pathways within the spinal cord, dorsal root ganglia and autonomic nervous system.
As a result, persistent inflammation or pain arising from one organ can sensitise neighbouring organs and surrounding muscles. This process is known as cross-organ sensitisation or viscero-visceral cross-sensitisation and helps explain why patients frequently develop overlapping bowel, bladder and pelvic pain symptoms.
Viscero-Visceral Cross-Sensitisation
Visceral organs send sensory information into shared spinal cord segments. When one organ becomes chronically inflamed, irritated or painful, the spinal cord neurons processing those signals can become increasingly excitable. Over time, neighbouring organs using similar neural pathways may also become hypersensitive.
This means that pathology in one organ may eventually produce symptoms in another organ even when the second organ appears structurally normal. For example, endometriosis affecting the uterus or pelvic peritoneum may increase sensitivity within the bowel or bladder. Similarly, chronic bowel inflammation may contribute to pelvic floor pain or bladder urgency.
This phenomenon is strongly supported by both experimental and clinical research and helps explain why conditions such as IBS, endometriosis, bladder pain syndrome and chronic pelvic pain commonly overlap.
Why One Organ Can Sensitise Another
The nervous system does not process visceral pain in a perfectly organ-specific way. Sensory neurons from different pelvic and abdominal organs converge onto shared spinal pathways. Repeated nociceptive input can therefore “spill over” into neighbouring neural circuits.
Persistent inflammation, mast cell activation, immune signalling and autonomic dysregulation may further amplify this process. Over time, the spinal cord and brain become increasingly efficient at generating pain responses, even when the original structural trigger has improved.
This is one reason why chronic pelvic pain often evolves into a much broader syndrome involving bowel symptoms, bladder pain, sexual pain, pelvic floor spasm, fatigue, sleep disturbance and widespread sensitisation.
Bowel–Bladder–Uterus Neural Convergence
The bowel, bladder and reproductive organs share overlapping autonomic and sensory innervation through the hypogastric plexus, pelvic plexus, sacral pathways and dorsal root ganglia. Signals from these organs converge within the spinal cord before being interpreted by higher brain centres.
Because of this neural convergence, patients with endometriosis commonly develop bowel symptoms, patients with bladder pain syndrome frequently have IBS-type symptoms, and patients with chronic bowel inflammation may develop pelvic floor dysfunction or bladder sensitivity.
The nervous system effectively becomes “trained” into a persistent state of heightened vigilance and reactivity across the entire pelvic region.
Pelvic Cross-Talk and Cross-Organ Sensitisation
IBD
Diverticular disease
Urgency
Pelvic pressure
Pelvic pain
Dysmenorrhoea
Why Pain Persists After “Successful” Surgery
Patients are often told that surgery was technically successful, inflammation has resolved or imaging now looks reassuring — yet the pain persists. This can be confusing and distressing for both patients and clinicians.
Cross-organ sensitisation and central amplification provide an important explanation for this phenomenon. Once the nervous system has become sensitised, removing the original structural lesion may not immediately reverse the abnormal pain processing that has developed within the spinal cord and brain.
This does not mean surgery “failed” or that the pain is psychological. It means the nervous system itself has become part of the ongoing pain process.
This is particularly relevant in endometriosis, chronic pelvic pain, bladder pain syndrome and persistent post-inflammatory bowel pain, where sensitisation can continue long after the original pathology has improved.
Myofascial Amplification and Pelvic Floor Dysfunction
Persistent visceral pain frequently leads to secondary muscle guarding within the abdominal wall, pelvic floor, obturator internus, piriformis and surrounding myofascial structures. Over time, these muscles may become hypertonic, painful and themselves capable of generating ongoing nociceptive input.
This creates a self-perpetuating cycle in which visceral sensitisation triggers pelvic floor spasm, and pelvic floor spasm further amplifies visceral pain. Patients may develop pain with sitting, bowel movements, bladder filling, intercourse or physical activity.
Addressing chronic pelvic pain therefore often requires a broader strategy that includes treatment of the nervous system, autonomic dysregulation, myofascial dysfunction and central sensitisation — not simply treatment of a single organ in isolation.
Key Clinical Message
In chronic abdominal and pelvic pain, organs frequently sensitise one another through shared neural pathways. This helps explain why bowel, bladder, pelvic floor and reproductive symptoms often coexist — and why successful management usually requires a multidisciplinary approach addressing both peripheral and central pain mechanisms.
Clinical Features of Visceral Hypersensitivity
Visceral hypersensitivity can present in different ways, but the core clinical pattern is pain that appears disproportionate to the visible structural findings. Patients may have normal or reassuring investigations, or an organic condition that has been treated, yet they continue to experience significant pain, bloating, urgency, nausea or pelvic discomfort.
The symptoms can range from localised visceral hypersensitivity, where internal organ sensations are amplified, to a broader central sensitisation state involving fatigue, sleep disturbance, brain fog, widespread pain and multisensory sensitivity.
Pain Characteristics
Visceral pain is often described as deep, dull, aching, cramping or pressure-like. It is frequently poorly localised and may move or fluctuate in intensity. Unlike abdominal wall pain, which is often sharply localised to a small tender point, visceral hypersensitivity often produces a more diffuse and difficult-to-pinpoint discomfort.
Some patients also describe burning, shooting or neuropathic-type symptoms, particularly when peripheral nerves, pelvic nerves or central sensitisation are involved.
Pain Triggered by Normal Physiological Events
A major clue to visceral hypersensitivity is pain triggered by normal internal activity. Eating, bowel movement, bladder filling, menstruation, sexual activity or pelvic organ distension may provoke disproportionate pain.
This happens because the threshold for perceiving visceral signals has fallen. Sensations that would normally be mild, temporary or barely noticed are interpreted by the nervous system as painful or threatening.
Bloating, Urgency and Nausea
Bloating is common because normal intestinal distension during digestion may be perceived as excessive pressure or pain. Patients may feel severely bloated even when objective distension is not marked.
Urgency can occur when the bowel or bladder becomes hypersensitive to filling. Nausea may accompany centrally mediated abdominal pain, especially when the autonomic nervous system and brain–gut pathways are involved.
Food-Related Pain
Some patients notice that particular foods trigger abdominal pain, bloating, cramping or urgency. This does not always mean a true allergy is present. In some cases, previous inflammation, altered gut permeability, mast cell activation or microbiome changes may make the gut more reactive to food-related stimuli.
Food-related symptoms are particularly relevant in IBS, post-infectious gut syndromes and some patients with inflammatory bowel disease in remission. Dietary approaches may help selected patients, but overly restrictive diets should be avoided unless supervised appropriately.
Abdominal Allodynia and Hyperalgesia
Abdominal allodynia means pain from a stimulus that should not normally be painful, such as light brushing of the skin. This can be tested gently by brushing the fingertips across the abdomen before deeper palpation.
Hyperalgesia means an exaggerated pain response to a mildly painful stimulus. In visceral hypersensitivity, patients may be unusually tender to light or moderate pressure, and the painful area may extend beyond the original organ or site of pathology.
Diffuse abdominal allodynia is particularly important because it suggests that central sensitisation may be contributing to the patient’s pain experience.
Fatigue, Brain Fog and Sleep Disturbance
When visceral hypersensitivity progresses into a broader central sensitisation state, patients may develop symptoms beyond the abdomen or pelvis. These can include fatigue, unrefreshing sleep, cognitive difficulty or “brain fog”, low mood and reduced ability to function day to day.
These symptoms are not separate from the pain problem. They reflect wider nervous system dysregulation involving pain-processing circuits, autonomic pathways, immune signalling and stress-regulation systems.
Multisensory Sensitivity
Some patients become sensitive not only to pain, but also to light, sound, smell, temperature, touch or motion. This multisensory sensitivity suggests that the central nervous system has become more reactive overall.
This pattern is often seen in patients with overlapping pain syndromes such as fibromyalgia, migraine, chronic pelvic pain, temporomandibular disorder, chronic fatigue-type presentations and other central sensitivity syndromes.
Opioid-Induced Hyperalgesia
Opioids can sometimes worsen centrally mediated abdominal or pelvic pain over time. When pain escalates despite increasing opioid doses, opioid-induced hyperalgesia or narcotic bowel syndrome should be considered.
In this situation, the nervous system becomes more sensitive rather than less sensitive. This is one reason why long-term opioids are generally avoided in visceral hypersensitivity and centrally mediated abdominal pain.
The clinical presentation often evolves from organ-specific visceral sensitivity to a wider central sensitisation pattern.
| Feature | Peripheral Visceral Hypersensitivity | Full Central Sensitisation / Nociplastic Pain |
|---|---|---|
| Pain location | Mainly abdominal, pelvic, bladder or gut-related | May spread beyond the original organ to the back, pelvis, limbs or widespread body regions |
| Triggers | Eating, bowel movement, bladder filling, menses, visceral distension | Pain may be triggered by touch, stress, poor sleep, activity, temperature, sound or emotional distress |
| Associated symptoms | Bloating, urgency, nausea, early satiety, cramping | Fatigue, brain fog, unrefreshing sleep, mood disturbance and multisensory sensitivity |
| Examination findings | Diffuse visceral tenderness; negative Carnett’s sign may support visceral origin | Abdominal allodynia, widespread hyperalgesia and tenderness beyond the original pain site |
| Relationship to investigations | Symptoms may be disproportionate to structural findings | Pain may persist despite successful treatment, remission or reassuring imaging |
| Overlapping conditions | IBS, functional dyspepsia, bladder pain syndrome, endometriosis | Fibromyalgia, migraine, chronic pelvic pain, TMJ pain, chronic fatigue-type symptoms |
| Medication response | May respond to gut-directed treatment, dietary strategies and low-dose neuromodulators | Often requires multimodal treatment including neuromodulators, behavioural therapy, pacing and nervous system regulation |
| Opioid effect | Limited role; risk of bowel dysfunction | May worsen pain through opioid-induced hyperalgesia or narcotic bowel syndrome |
Key Clinical Message
The most important clinical clue is disproportionate pain: symptoms that are more severe, persistent or widespread than expected from the visible structural findings. When fatigue, sleep disturbance, abdominal allodynia, multisensory sensitivity or multiple overlapping pain conditions are present, central sensitisation should be considered.
Diagnosing Visceral Hypersensitivity
Diagnosing visceral hypersensitivity is often challenging because there is no single blood test, scan or investigation that definitively confirms the condition. In routine clinical practice, the diagnosis is largely based on careful clinical assessment, exclusion of important structural pathology and recognition of characteristic pain-processing patterns.
A key principle is that visceral hypersensitivity should never simply be assumed. Appropriate gastrointestinal, gynaecological, urological, musculoskeletal and abdominal wall causes must first be considered based on the patient’s symptoms, examination findings and risk factors.
Why It Is Primarily a Clinical Diagnosis
The gold-standard research test for visceral sensitivity is the rectal or colonic barostat, which measures pain thresholds to controlled balloon distension. However, this is not routinely available in standard clinical practice.
As a result, diagnosis relies heavily on identifying a recognisable clinical pattern. This includes disproportionate pain, symptoms triggered by normal physiological activity, diffuse or poorly localised visceral pain, abdominal allodynia and overlapping features of central sensitisation.
The diagnosis becomes more likely when structural investigations are reassuring or when symptoms persist despite appropriate treatment of the original pathology.
Excluding Structural Pathology
Before considering visceral hypersensitivity, clinicians must assess for structural, inflammatory, infective, malignant and surgical causes of abdominal or pelvic pain. The investigations required depend on the clinical scenario and may include blood tests, stool testing, ultrasound, CT, MRI, endoscopy, colonoscopy, pelvic imaging or specialist assessment.
Importantly, the presence of structural pathology does not exclude visceral hypersensitivity. Many patients have a combination of organic disease and altered pain processing. For example, patients with endometriosis, diverticular disease or inflammatory bowel disease may continue to experience significant pain despite technically successful treatment or remission.
The Importance of Pain–Pathology Mismatch
One of the strongest clues to visceral hypersensitivity is a mismatch between symptom severity and visible pathology. The patient’s pain appears much greater than would normally be expected from the structural findings alone.
Examples include severe pelvic pain with minimal endometriosis, persistent abdominal pain after resolved diverticulitis, ongoing bowel pain despite inflammatory bowel disease remission or disabling pain despite reassuring imaging and investigations.
This mismatch does not imply exaggeration or psychological causation. It reflects altered peripheral and central pain processing.
Carnett’s Sign Explained
Carnett’s sign is an important bedside examination manoeuvre used to distinguish abdominal wall pain from visceral pain. It is particularly useful because abdominal wall pain is commonly overlooked and may mimic visceral disease.
The examiner identifies the point of maximal tenderness while the patient lies relaxed. The patient is then asked to tense the abdominal wall by lifting the head or raising the legs while the tender area is re-palpated.
Positive Carnett’s sign: pain remains the same or worsens when the abdominal muscles tense. This suggests the pain arises from the abdominal wall or myofascial structures.
Negative Carnett’s sign: pain improves when the abdominal wall is tensed. This suggests a visceral source because the tightened abdominal muscles protect the internal organs from deeper palpation.
Distinguishing visceral pain from abdominal wall pain is one of the most important steps in assessing chronic abdominal pain.
| Feature | Visceral Pain | Abdominal Wall Pain |
|---|---|---|
| Pain location | Diffuse, vague, poorly localised | Small, sharply localised tender area |
| Carnett’s sign | Negative — pain improves with muscle tensing | Positive — pain worsens or stays the same |
| Associated symptoms | Bloating, urgency, nausea, bowel or bladder symptoms | Usually absent |
| Pain triggers | Eating, bowel movement, bladder filling, menstruation | Movement, posture, coughing, abdominal muscle use |
| Allodynia pattern | Diffuse abdominal sensitivity | Localised trigger point tenderness |
| Response to trigger point injection | Limited or inconsistent | Often significant improvement |
ACNES and Myofascial Pain
Anterior cutaneous nerve entrapment syndrome (ACNES) is one of the most common causes of chronic abdominal wall pain. It occurs when small cutaneous nerves become trapped as they pass through the abdominal wall.
Patients often describe a small, localised area of sharp or burning pain that worsens with movement, posture or muscle activation. Trigger point injections may be both diagnostic and therapeutic.
Myofascial pain involving the abdominal wall or pelvic floor may also coexist with visceral hypersensitivity and contribute to ongoing pain amplification.
Central Sensitisation Inventory (CSI)
The Central Sensitisation Inventory (CSI) is a validated questionnaire used to screen for symptoms associated with central sensitisation. It asks about fatigue, sleep disturbance, cognitive symptoms, sensory sensitivity, widespread pain and other central nervous system features.
A higher CSI score suggests a greater likelihood that central sensitisation is contributing to the patient’s symptoms. The tool does not diagnose a single disease but helps identify broader nervous system amplification.
Typical CSI Interpretation
| CSI Score | Interpretation |
|---|---|
| 0–29 | Low likelihood of significant central sensitisation |
| 30–39 | Borderline or mild central sensitisation features |
| 40–49 | Clinically significant central sensitisation likely |
| 50+ | High symptom burden with strong central amplification features |
Quantitative Sensory Testing
Quantitative sensory testing (QST) uses controlled thermal or mechanical stimuli to assess pain thresholds and sensory processing. It is mainly used in specialist or research settings.
Abnormal findings may demonstrate peripheral sensitisation, central sensitisation or impaired pain modulation.
Rectal Barostat Testing
Rectal barostat testing is considered the gold-standard research method for assessing visceral sensitivity. A balloon device is used to apply graded distension within the rectum or colon while sensory thresholds are measured.
Patients with visceral hypersensitivity often demonstrate reduced pain thresholds compared with healthy controls. However, this test is not routinely available outside specialist research centres.
Conditioned Pain Modulation Testing
Conditioned pain modulation (CPM) assesses the nervous system’s ability to inhibit pain. In healthy individuals, one painful stimulus can partially suppress another painful stimulus — often described as “pain inhibits pain”.
In central sensitisation states, this inhibitory system may function poorly, allowing pain signals to become amplified and persistent.
Practical Diagnostic Pathway
Key Clinical Message
Visceral hypersensitivity is primarily diagnosed through careful clinical assessment and recognition of characteristic pain-processing patterns. The most important clues are disproportionate pain, symptoms triggered by normal physiological events, negative structural investigations and evidence of central sensitisation.
Red Flags and When Further Investigation Is Needed
Although visceral hypersensitivity and central sensitisation are important causes of chronic abdominal and pelvic pain, it is extremely important not to assume that all symptoms are “functional” or purely related to pain sensitisation.
Patients with persistent abdominal or pelvic symptoms still require careful assessment for inflammatory, infective, structural, neurological, vascular and malignant conditions. Visceral hypersensitivity should only be considered after appropriate evaluation based on the clinical context.
Importantly, patients may also have a combination of structural pathology and sensitisation at the same time. The presence of visceral hypersensitivity does not exclude organic disease.
Red Flag Features Requiring Further Assessment
| Red Flag | Why It Matters | Examples of Concern |
|---|---|---|
| Unintentional weight loss | May suggest malignancy, inflammatory disease, malabsorption or significant systemic illness | Cancer, inflammatory bowel disease, pancreatic disease, chronic infection |
| GI bleeding | Visible or occult bleeding requires investigation | Rectal bleeding, melaena, anaemia, blood mixed with stool |
| Persistent fever or raised inflammatory markers | May indicate active inflammation, infection or autoimmune disease | Abscess, active IBD, pelvic infection, systemic inflammatory disease |
| Progressive neurological symptoms | Neurological deficit requires urgent evaluation | Weakness, numbness, bowel/bladder dysfunction, gait disturbance |
| New-onset symptoms in older age | Organic pathology becomes more likely with age | New bowel symptoms, unexplained abdominal pain, altered bowel habit |
| Persistent vomiting or severe dysphagia | May indicate obstruction or serious upper GI pathology | Upper GI malignancy, obstruction, severe motility disorder |
| Palpable abdominal or pelvic mass | Requires structural investigation | Malignancy, large fibroid, ovarian pathology, inflammatory mass |
| Family history of GI malignancy or IBD | May alter investigation thresholds | Colorectal cancer, Crohn’s disease, ulcerative colitis |
Weight Loss
Unintentional weight loss should never simply be attributed to visceral hypersensitivity. Significant or progressive weight loss may suggest inflammatory bowel disease, malignancy, pancreatic disease, malabsorption, chronic infection or severe systemic illness.
Although some patients reduce food intake because eating becomes painful, this explanation should only be accepted after appropriate medical assessment.
GI Bleeding
Visible rectal bleeding, melaena, unexplained iron deficiency anaemia or blood mixed within stool requires further investigation. These findings are not typical features of visceral hypersensitivity itself.
Possible causes include inflammatory bowel disease, colorectal pathology, diverticular bleeding, haemorrhoids, upper GI bleeding and malignancy.
Fever and Inflammatory Markers
Persistent fever, night sweats or significantly raised inflammatory markers suggest active inflammatory or infective pathology rather than isolated sensitisation.
Examples include abscess formation, inflammatory bowel disease flare, pelvic infection, pancreatitis or systemic inflammatory disease.
Progressive Neurological Symptoms
Progressive weakness, numbness, saddle sensory change, gait disturbance or bowel/bladder dysfunction should always prompt urgent neurological assessment.
These symptoms may indicate spinal cord, nerve root or serious neurological pathology rather than visceral hypersensitivity.
Malignancy Red Flags
New-onset symptoms later in life, progressive symptoms, unexplained anaemia, palpable masses, persistent vomiting or a strong family history of gastrointestinal malignancy require careful investigation.
Although visceral hypersensitivity may coexist with cancer-related pain or post-treatment pain states, malignancy should not be missed by prematurely assuming a functional diagnosis.
When Not to Assume “Functional Pain”
- Rapidly progressive or severe new symptoms
- Significant weight loss or systemic illness
- Persistent GI bleeding or unexplained anaemia
- Marked inflammatory marker elevation
- Progressive neurological symptoms
- Palpable abdominal or pelvic mass
- Persistent vomiting or dysphagia
- Symptoms clearly outside the expected pattern of visceral hypersensitivity
Key Clinical Message
Visceral hypersensitivity is a recognised pain-processing disorder, but it remains a diagnosis that should be made carefully and responsibly. Red flag symptoms always require appropriate investigation, and patients may have both structural pathology and nervous system sensitisation at the same time.
Principles of Treatment
Treating visceral hypersensitivity requires a broader approach than simply looking for a single structural abnormality to “fix”. Once pain pathways become sensitised, the nervous system itself becomes part of the ongoing problem.
Effective treatment therefore aims to calm both the peripheral drivers arising from the gut, pelvis or abdominal wall and the central amplification occurring within the spinal cord, brain and autonomic nervous system.
This is why successful management usually involves a multimodal strategy combining medical treatment, nervous system regulation, lifestyle modification, physical rehabilitation, psychological support and, in selected patients, interventional pain procedures.
Why Multimodal Treatment Is Essential
Visceral hypersensitivity is rarely caused by a single mechanism alone. Patients may simultaneously have low-grade inflammation, mast cell activation, pelvic floor dysfunction, altered autonomic regulation, central sensitisation, sleep disturbance and psychological stress amplification.
Because multiple biological systems are involved, treatment focused on only one component is often insufficient. For example, treating bowel inflammation alone may not fully reverse established central sensitisation, while psychological therapy alone may not adequately address ongoing peripheral nociceptive input.
The aim is therefore not simply symptom suppression, but gradual downregulation of the sensitised nervous system while improving function, resilience and quality of life.
Core Components of Multimodal Treatment
Peripheral Drivers
Managing inflammation, gut triggers, pelvic floor dysfunction, abdominal wall pain and autonomic contributors.
Central Sensitisation
Neuromodulators, sleep restoration, pacing, nervous system regulation and behavioural therapies.
Physical Rehabilitation
Pelvic floor therapy, myofascial treatment, gradual reconditioning and movement rehabilitation.
Psychological Support
Stress regulation, trauma-informed care, CBT, ACT and reducing fear-based pain amplification.
Treating Peripheral and Central Mechanisms Together
A major treatment principle is that both peripheral and central mechanisms often need to be addressed simultaneously. Persistent nociceptive input from the bowel, bladder, abdominal wall or pelvic floor can continue to reinforce spinal cord and brain sensitisation.
For example, patients with endometriosis may benefit from treatment of residual pelvic inflammation while also addressing pelvic floor dysfunction, sleep disturbance and central amplification. Similarly, patients with IBS may require dietary management alongside neuromodulator therapy and behavioural interventions targeting the brain–gut axis.
When only one component is treated, patients may experience temporary or incomplete improvement because the wider sensitisation network remains active.
Treatment Philosophy
Why Opioids Often Make Things Worse
Although opioids may occasionally provide short-term relief during severe acute pain episodes, long-term opioid therapy is generally problematic in visceral hypersensitivity and centrally mediated abdominal pain.
Opioids can slow gut motility, worsen constipation, increase bloating and impair gastrointestinal function. More importantly, prolonged opioid exposure may increase pain sensitivity through opioid-induced hyperalgesia.
Some patients develop narcotic bowel syndrome, where abdominal pain paradoxically worsens despite escalating opioid doses. In this situation, the nervous system becomes increasingly sensitised rather than calmer.
This is why modern management strategies increasingly focus on neuromodulation and nervous system regulation rather than long-term opioid escalation.
Why Long-Term Opioids Are Often Avoided
- Can worsen constipation and gut dysmotility
- May increase bloating and nausea
- Risk of opioid-induced hyperalgesia
- May reinforce central sensitisation
- Tolerance often develops over time
- Can impair functional recovery and quality of life
The Importance of Patient Education
Patient education is one of the most important components of treatment. Many patients have previously been told that investigations are “normal”, leading them to feel dismissed or misunderstood.
Understanding that visceral hypersensitivity is a recognised neuroimmune pain-processing disorder can itself reduce fear and catastrophisation. Patients often improve when they understand that the symptoms are biologically real, even when scans appear reassuring.
Education should also explain that stress, poor sleep and emotional overload do not mean the pain is imaginary. These factors influence the nervous system and brain–gut axis in measurable biological ways.
Realistic Expectations and Functional Recovery
Patients with long-standing visceral hypersensitivity often hope for a single intervention that will completely eliminate symptoms. Unfortunately, once sensitisation becomes established, recovery is usually gradual rather than immediate.
The aim of treatment is typically to reduce pain intensity, improve function, restore confidence, improve sleep, increase activity tolerance and reduce nervous system reactivity over time.
Fluctuations and temporary setbacks are common and do not necessarily mean treatment is failing. In many patients, meaningful progress occurs through gradual nervous system recalibration rather than through a single “curative” procedure.
Key Clinical Message
Successful treatment of visceral hypersensitivity requires a multimodal approach addressing both peripheral and central pain mechanisms. Long-term improvement usually comes from gradual nervous system downregulation, improved function and better pain modulation rather than from a single isolated treatment.
Neuromodulator Medications
Neuromodulator medications are one of the most important treatment strategies in visceral hypersensitivity and centrally mediated abdominal or pelvic pain. These medications do not simply “mask” pain. Their aim is to reduce abnormal nervous system amplification and improve pain modulation within the gut–brain axis, spinal cord and central nervous system.
Importantly, these medications are often used at lower doses than in psychiatry. Although some were originally developed as antidepressants or anticonvulsants, their role in visceral pain is related primarily to pain modulation, autonomic regulation and reduction of sensory hypersensitivity.
Response varies significantly between individuals. Patients with more prominent central sensitisation, poor sleep, widespread pain or autonomic dysregulation often require a broader neuromodulatory approach rather than gut-directed treatment alone.
Tricyclic Antidepressants (Amitriptyline/Nortriptyline)
Low-dose tricyclic antidepressants remain among the best-studied medications for visceral hypersensitivity and IBS-related pain. Amitriptyline and nortriptyline work partly by enhancing descending pain inhibition within the spinal cord and reducing abnormal sensory amplification.
They may improve abdominal pain, sleep quality, visceral sensitivity and autonomic hyperarousal. Lower doses are typically used than in major depressive disorder.
Amitriptyline tends to be more sedating and may be helpful in patients with insomnia or hyperarousal, whereas nortriptyline is often slightly better tolerated with fewer anticholinergic effects.
Typical starting approach
Amitriptyline is often started at 5–10 mg at night and increased gradually depending on benefit and tolerability.
SNRIs (Duloxetine/Venlafaxine)
SNRIs enhance both serotonin and noradrenaline signalling and may improve central pain modulation. Duloxetine is particularly useful when visceral hypersensitivity overlaps with fibromyalgia, chronic pelvic pain, widespread pain or neuropathic symptoms.
These medications may help patients with significant central sensitisation, fatigue, anxiety, hypervigilance or multisystem pain amplification.
Some patients experience nausea, sweating, activation or insomnia early in treatment, so gradual titration is important.
Pregabalin and Gabapentin
Gabapentinoids reduce neuronal excitability and may help patients with prominent hyperalgesia, allodynia, neuropathic-type pain or pelvic floor hypertonicity.
Pregabalin has been studied in visceral pain states and may reduce visceral sensitivity as well as anxiety-related hyperarousal. These medications are often particularly useful in patients with widespread central sensitisation and sleep disturbance.
Common side effects include sedation, dizziness, cognitive slowing and weight gain. Careful titration is important to minimise adverse effects.
Buspirone and Functional Dyspepsia
Buspirone is a serotonin 5-HT1A partial agonist traditionally used for anxiety disorders, but it may also improve symptoms in functional dyspepsia.
Its potential benefit appears related to improved gastric accommodation and modulation of upper gastrointestinal sensory processing. Some patients report improvement in postprandial fullness, upper abdominal discomfort and meal-related symptoms.
Buspirone may be particularly useful when upper GI hypersensitivity overlaps with autonomic arousal or anxiety-related symptom amplification.
Mirtazapine
Mirtazapine is sometimes used in patients with visceral hypersensitivity who also have poor sleep, nausea, weight loss or reduced appetite. It has antihistaminergic and serotonergic effects and may help regulate sleep and autonomic overactivity.
Because it can stimulate appetite and improve sleep, it may be particularly useful in selected patients with functional dyspepsia, upper GI symptoms or severe sleep disturbance.
Sedation and weight gain are common side effects.
Low-Dose Antipsychotic Augmentation
In highly selected refractory cases, very low-dose antipsychotic augmentation may occasionally be considered by experienced clinicians, particularly when severe insomnia, autonomic hyperarousal, functional nausea or extreme nervous system activation are present.
These medications are not first-line therapies and should be used cautiously because of metabolic, neurological and sedative side effects. Their role is generally limited to complex refractory cases under specialist supervision.
Practical Prescribing Principles
One of the most important principles in treating visceral hypersensitivity is to “start low and go slow”. Patients with sensitised nervous systems are often unusually sensitive to medication side effects.
Starting with very small doses and increasing gradually usually improves tolerability and long-term adherence. Patients should also be warned that early side effects often improve with time.
No single medication works for everyone. Treatment frequently involves careful trial-and-error guided by the dominant symptom pattern, sleep quality, autonomic symptoms, mood, bowel habit and degree of central sensitisation.
Neuromodulators are chosen based on the dominant symptom pattern, sleep disturbance, autonomic features and degree of central sensitisation.
| Medication | Mechanism | Best Evidence / Typical Use | Common Side Effects |
|---|---|---|---|
| Amitriptyline | Enhances descending pain inhibition; sedative effect | IBS pain, sleep disturbance, central sensitisation | Dry mouth, constipation, sedation, weight gain |
| Nortriptyline | Similar to amitriptyline with fewer anticholinergic effects | Visceral pain with poor TCA tolerability | Dry mouth, dizziness, sedation |
| Duloxetine | SNRI-mediated central pain modulation | Fibromyalgia overlap, pelvic pain, widespread sensitisation | Nausea, sweating, insomnia, reduced appetite |
| Pregabalin | Reduces neuronal excitability | Hyperalgesia, allodynia, sleep disturbance, pelvic pain | Sedation, dizziness, weight gain |
| Gabapentin | Calcium channel modulation | Neuropathic features and central sensitisation | Sedation, dizziness, cognitive slowing |
| Buspirone | 5-HT1A partial agonist; improves gastric accommodation | Functional dyspepsia and meal-related symptoms | Dizziness, headache, nausea |
| Mirtazapine | Serotonergic and antihistaminergic modulation | Sleep disturbance, nausea, appetite loss | Sedation, weight gain, increased appetite |
Side Effects and Titration
Patients with central sensitisation often experience side effects at lower doses than expected. Rapid escalation frequently worsens tolerability and may increase fear of medication.
Gradual titration, realistic counselling and regular review are therefore extremely important. Some patients may require weeks before meaningful benefit develops.
The goal is usually improved pain modulation, sleep quality and function rather than complete elimination of every symptom.
Key Clinical Message
Neuromodulator medications work by calming abnormal pain amplification within the gut–brain axis and central nervous system. Successful prescribing usually requires careful individualisation, slow titration and realistic expectations rather than aggressive dose escalation.
Mast Cells, Histamine and Antihistamine Therapies
Increasing evidence suggests that mast cells and histamine signalling may play an important role in visceral hypersensitivity and disorders of gut–brain interaction. Although this area remains biologically complex and not fully understood, neuroimmune activation appears to contribute to abnormal visceral pain signalling in at least a subgroup of patients.
This does not mean that all patients with IBS or chronic abdominal pain have mast cell activation syndrome. However, mast cell–nerve interactions are increasingly recognised as one mechanism capable of amplifying visceral sensitivity, bloating, urgency and abdominal pain.
The greatest relevance of this section is not necessarily the diagnosis of a specific mast cell disorder, but the recognition that immune signalling and nervous system sensitisation are closely linked.
Mast Cell Activation and Visceral Pain
Mast cells are immune cells located throughout the gastrointestinal tract and pelvic tissues. They are often found in close proximity to sensory nerve fibres, allowing direct communication between the immune system and the nervous system.
When activated, mast cells release histamine, cytokines, prostaglandins, tryptase and other inflammatory mediators. These substances can lower the activation threshold of visceral sensory nerves, making the gut or pelvic organs more sensitive to stretch, pressure and chemical stimuli.
Increased mast cell density and mast cell activation have been demonstrated in subsets of patients with IBS, functional dyspepsia and chronic pelvic pain syndromes. The proximity of mast cells to enteric nerves appears particularly important because it may directly amplify visceral pain signalling.
How Mast Cells May Amplify Visceral Pain
Histamine Pathways
Histamine acts through multiple receptor systems and has effects on sensory nerves, immune regulation, vascular tone and gastrointestinal function. Within the gut, histamine may increase visceral sensitivity and alter motility, secretion and neuroimmune signalling.
Histamine can also activate TRP channels and sensitise enteric nerves, creating a direct link between immune activation and pain amplification. This may contribute to abdominal pain, urgency, bloating and food-related symptom flares in susceptible patients.
H1 vs H4 Receptors
Different histamine receptors appear to play different roles in visceral hypersensitivity. H1 receptors are involved in classic histamine-related effects such as itching, vascular changes and sensory nerve activation. H1 receptor signalling may contribute to visceral pain amplification and sensory hypersensitivity.
H4 receptors are more closely linked to immune regulation and mast cell–mediated inflammatory signalling. Experimental research suggests that H4 receptor pathways may contribute to visceral hypersensitivity and neuroimmune activation within the gut.
Interest in H4 receptors is growing because they may represent a future therapeutic target in disorders of gut–brain interaction, although clinical evidence remains limited at present.
| Receptor | Main Role | Potential Relevance to Visceral Pain |
|---|---|---|
| H1 | Sensory nerve activation and vascular effects | Pain amplification, hypersensitivity, neurogenic inflammation |
| H4 | Immune and mast cell regulation | Neuroimmune activation and chronic visceral sensitisation |
Ketotifen
Ketotifen is both an H1 antihistamine and a mast cell stabiliser. Some studies suggest it may reduce visceral hypersensitivity and improve abdominal pain in selected patients with IBS.
The proposed mechanism involves stabilising mast cells and reducing the release of histamine and inflammatory mediators close to enteric nerves.
Sedation is a common side effect, and evidence remains limited. Ketotifen is therefore usually considered an adjunctive or specialist treatment rather than standard first-line therapy.
Ebastine
Ebastine is a second-generation H1 antihistamine that has attracted interest because of studies suggesting improvement in IBS-related abdominal pain and sensory hypersensitivity.
Experimental work suggests that H1 blockade may reduce nerve sensitisation and visceral pain amplification in certain patients. However, clinical evidence remains relatively early and larger studies are still needed.
At present, antihistamine approaches should generally be viewed as part of a broader multimodal strategy rather than as standalone treatments.
Antihistamines Beyond IBS
Although most research has focused on IBS, mast cell–nerve interactions may also be relevant in functional dyspepsia, chronic pelvic pain, bladder pain syndrome and post-infectious gut syndromes.
Some patients with broader central sensitisation or autonomic dysregulation appear particularly sensitive to food triggers, environmental triggers or inflammatory flares, raising the possibility of wider neuroimmune involvement.
However, evidence outside IBS remains limited and antihistamines should not be presented as universally effective treatments for chronic pain disorders.
Food Antigens and Mast Cell Activation
In some patients, food-related symptoms may partly reflect mast cell activation, altered intestinal permeability or abnormal neuroimmune signalling rather than classic IgE-mediated allergy.
Food antigens may interact with immune pathways within the gut wall, potentially increasing mast cell activation and sensitising nearby sensory nerves. This may contribute to meal-related pain, bloating, urgency or nausea.
Importantly, this area is still evolving scientifically. Excessively restrictive diets can sometimes worsen nutrition, fear of eating and symptom hypervigilance, so dietary interventions should be approached carefully.
Important Clinical Caution
Mast cell involvement in visceral hypersensitivity does not automatically mean that a patient has mast cell activation syndrome (MCAS).
The science around neuroimmune activation is still evolving, and antihistamines are not universal cures for IBS or chronic abdominal pain.
These therapies are best viewed as adjunctive tools within a broader multimodal treatment strategy targeting both peripheral and central sensitisation.
Emerging Therapies (Investigational)
Several emerging therapies are being investigated for their potential role in neuroimmune signalling and visceral pain modulation. At present, these approaches remain experimental and are not established standard treatments.
| Emerging Therapy | Theoretical Mechanism | Current Status |
|---|---|---|
| PAR-2 antagonists | Reduce protease-mediated sensory nerve activation | Early experimental research |
| H4 antagonists | Target neuroimmune and mast cell pathways | Investigational; limited clinical data |
| CGRP-targeted approaches | Modulate neurogenic inflammation and sensory signalling | Primarily migraine-focused at present |
Key Clinical Message
Mast cells and histamine pathways may contribute to visceral hypersensitivity by sensitising enteric nerves and amplifying neuroimmune signalling. Although antihistamine and mast cell–targeted therapies may help selected patients, evidence remains evolving and these treatments should be integrated into a broader multimodal pain-management approach.
Low Dose Naltrexone (LDN)
Low dose naltrexone, often abbreviated to LDN, is an emerging treatment that has attracted interest in chronic pain conditions associated with central sensitisation, neuroimmune activation and altered pain modulation. It is not a conventional analgesic and should not be viewed as a quick painkiller. Its proposed role is to gently modulate immune–nervous system signalling over time.
In visceral hypersensitivity, LDN is of interest because many patients have overlapping features of central sensitisation, autonomic dysregulation, fatigue, sleep disturbance, fibromyalgia-type symptoms or neuroimmune activation. However, the evidence base remains evolving, and LDN should be presented as a possible adjunctive option rather than an established first-line treatment.
Proposed Mechanisms
At standard doses, naltrexone blocks opioid receptors and is used in addiction medicine. At much lower doses, usually in the range of 1–4.5 mg daily, it appears to have different biological effects. These may include modulation of microglial activity, reduction of pro-inflammatory signalling and improved endogenous pain inhibition.
One theory is that short-lived opioid receptor blockade may lead to a rebound increase in the body’s own endorphin activity. Another proposed mechanism is reduced activation of toll-like receptor 4 pathways on immune cells and microglia, which may help calm neuroinflammation.
Microglial Modulation
Microglia are immune-like cells within the central nervous system. When persistently activated, they can release inflammatory mediators that amplify pain pathways and contribute to central sensitisation.
LDN is thought to have a potential microglial-modulating effect. This is why it has been explored in conditions where pain appears to be maintained by neuroimmune activation, including fibromyalgia, chronic fatigue-type syndromes, neuropathic pain states and some complex chronic pain presentations.
How LDN May Help Sensitised Pain States
Evidence in Central Sensitisation Disorders
The most commonly discussed evidence for LDN comes from central sensitisation conditions such as fibromyalgia and complex chronic pain states. Some small studies and clinical reports suggest improvements in pain, fatigue, mood and quality of life, although larger high-quality trials are still needed.
LDN has also been discussed in conditions such as chronic fatigue syndrome, Long COVID, neuropathic pain and inflammatory pain states. The scientific rationale is strongest where neuroimmune activation and central sensitisation appear to be major contributors.
At present, LDN should be described as a promising but still evolving treatment option rather than a proven universal therapy.
Potential Role in Visceral Hypersensitivity
There is interest in LDN for visceral hypersensitivity because chronic abdominal and pelvic pain often involves neuroimmune activation, central sensitisation, autonomic dysregulation and overlapping pain syndromes.
Patients who may be considered for LDN are those with prominent central sensitisation features, such as widespread pain, fatigue, unrefreshing sleep, brain fog, fibromyalgia overlap, Long COVID-type symptoms or poor tolerance of standard neuromodulators.
LDN is unlikely to be sufficient as a standalone treatment when there is active inflammatory disease, untreated structural pathology, severe pelvic floor dysfunction or ongoing abdominal wall pain. It is best considered as one part of a broader multimodal plan.
| Clinical Situation | Possible Relevance of LDN | Important Limitation |
|---|---|---|
| Fibromyalgia overlap | May help pain amplification and fatigue in selected patients | Evidence still limited; not universally effective |
| Visceral hypersensitivity with central sensitisation | May support neuroimmune downregulation | Should not replace assessment for structural disease |
| Long COVID-type symptom overlap | May be considered where fatigue, dysautonomia and pain sensitisation coexist | Evidence remains emerging |
| Active inflammatory or structural pathology | May have only adjunctive relevance | Primary disease treatment remains essential |
Practical Dosing
LDN is usually prescribed at much lower doses than standard naltrexone. A common approach is to start at 0.5–1 mg at night and increase gradually every 1–2 weeks depending on tolerance and response.
Many patients are titrated towards 3–4.5 mg daily, although some respond to lower doses and others cannot tolerate higher doses. Patients with marked medication sensitivity may need slower titration.
Clinical benefit, if it occurs, may take several weeks or months. It is usually assessed in terms of pain sensitivity, fatigue, sleep, function and overall symptom burden rather than immediate analgesia.
Example Titration Approach
- Start: 0.5–1 mg at night
- Increase gradually every 1–2 weeks if tolerated
- Common target range: 3–4.5 mg at night
- Use slower titration in medication-sensitive patients
- Assess response over several weeks rather than days
Side Effects and Safety
LDN is generally considered well tolerated, but side effects can occur. These may include vivid dreams, sleep disturbance, headache, nausea, irritability or temporary symptom fluctuation during dose changes.
Because naltrexone blocks opioid receptors, it should not be used alongside opioid medication. Patients taking opioids, or likely to need opioid analgesia for surgery or acute pain, require careful medical advice before considering LDN.
LDN should be prescribed and monitored by a clinician familiar with its use, particularly in patients with complex medical conditions, liver disease, pregnancy, multiple medications or significant sensitivity to medication changes.
Key Clinical Message
LDN is a promising adjunctive treatment for selected patients with central sensitisation, neuroimmune activation and overlapping chronic pain symptoms. In visceral hypersensitivity, it should be viewed as part of a broader multimodal plan rather than a standalone cure.
Diet, Gut Microbiome and Lifestyle Factors
Diet, gut microbiome function, sleep, stress regulation and physical activity can all influence visceral hypersensitivity through effects on inflammation, autonomic balance, neuroimmune signalling and the brain–gut axis. Although lifestyle approaches are rarely “curative”, they may meaningfully reduce symptom amplification in selected patients.
Low-FODMAP Diet
The low-FODMAP diet has the strongest evidence among dietary approaches for IBS-related bloating, abdominal pain and altered bowel habit. It works by reducing fermentable carbohydrates that can increase intestinal distension and trigger symptoms in sensitive individuals.
Importantly, the diet is usually intended as a temporary structured elimination and reintroduction process rather than a lifelong highly restrictive diet.
Food Trigger Identification
Some patients identify reproducible symptom triggers related to particular foods, meal size or eating patterns. Keeping a symptom and food diary may occasionally help identify patterns.
However, excessive focus on food can sometimes increase anxiety, hypervigilance and fear-based eating behaviours, particularly in highly sensitised patients.
Elimination Diets
Elimination diets may help selected patients when there is suspicion of food-related symptom amplification, but overly restrictive diets should be approached cautiously.
Nutritional deficiency, microbiome disruption and worsening psychological stress around food can occur if diets become excessively restrictive without appropriate supervision.
Microbiome and Neuroimmune Signalling
The gut microbiome interacts closely with immune pathways, the enteric nervous system and the brain–gut axis. Altered microbiome composition may influence inflammation, mast cell activation, intestinal permeability and visceral sensitivity.
Although microbiome research is rapidly expanding, many mechanisms remain incompletely understood and routine microbiome testing is not currently recommended in standard clinical practice.
Probiotics
Some probiotic formulations may modestly improve bloating and IBS symptoms in selected patients, although results are inconsistent and strain-specific.
No single probiotic works for everyone, and benefits are often relatively modest rather than dramatic.
Rifaximin
Rifaximin is a minimally absorbed antibiotic that has evidence for selected patients with IBS, particularly IBS with bloating and diarrhoea-predominant symptoms.
The mechanism may involve microbiome modulation rather than treatment of overt infection. Response varies considerably between individuals.
Fecal Microbiota Transplantation (FMT)
FMT has attracted interest because of the growing recognition of microbiome involvement in gut–brain disorders. However, evidence in visceral hypersensitivity and IBS remains mixed and inconsistent.
At present, FMT should be regarded as investigational in this context and is not considered a routine treatment for visceral hypersensitivity.
| Approach | Potential Role | Important Caution |
|---|---|---|
| Low-FODMAP diet | May reduce bloating and IBS symptoms | Should not become permanently restrictive |
| Probiotics | May help selected patients | Benefits are strain-specific and variable |
| Rifaximin | Useful in some IBS-D presentations | Not universally effective |
| FMT | Investigational microbiome modulation | Evidence remains mixed and limited |
Sleep, Exercise and Stress Regulation
Poor sleep, chronic stress and physical deconditioning can all worsen central sensitisation and visceral symptom amplification. Sleep restoration, gradual exercise and nervous system regulation are therefore important components of long-term management.
The goal is not intense exercise or “pushing through pain”, but gradual improvement in nervous system resilience and functional tolerance over time.
Key Clinical Message
Dietary and lifestyle approaches may help reduce symptom amplification in selected patients, particularly when integrated into a broader multimodal strategy targeting the gut–brain axis, neuroimmune signalling and central sensitisation.
Brain–Gut Behavioural Therapies
Brain–gut behavioural therapies are increasingly recognised as important components of treatment in visceral hypersensitivity and disorders of gut–brain interaction. These approaches are not based on the idea that the pain is “imaginary”. Instead, they aim to reduce nervous system amplification, autonomic hyperarousal and maladaptive pain-processing patterns.
The gut and brain communicate continuously through neural, immune, hormonal and autonomic pathways. Stress, fear, hypervigilance and previous trauma can therefore influence visceral sensitivity in biologically measurable ways.
Brain–Gut Amplification Cycle
Cognitive Behavioural Therapy (CBT)
CBT aims to reduce unhelpful fear-based patterns, catastrophisation, symptom hypervigilance and avoidance behaviours that may amplify nervous system activation. It can also help patients improve pacing, coping strategies and functional recovery.
Importantly, CBT is not about convincing patients that the pain is psychological. The goal is to reduce the biological stress amplification that can worsen visceral sensitivity.
Gut-Directed Hypnotherapy
Gut-directed hypnotherapy has evidence in IBS and disorders of gut–brain interaction. It aims to reduce visceral hypervigilance and alter brain–gut processing through guided relaxation and focused imagery techniques.
Some patients experience meaningful improvement in abdominal pain, bloating and bowel symptoms, although response varies.
Acceptance and Commitment Therapy (ACT)
ACT focuses less on eliminating symptoms completely and more on reducing the struggle with pain while improving psychological flexibility and meaningful functional engagement.
This approach may be particularly helpful in long-standing sensitisation states where fear, avoidance and nervous system hyperreactivity have become deeply established.
Mindfulness-Based Therapies
Mindfulness-based approaches aim to reduce autonomic arousal and excessive threat monitoring. They may help some patients become less reactive to symptom fluctuations and improve nervous system regulation.
Benefits are often gradual and are usually greatest when integrated into a broader multimodal management strategy.
Pain Reprocessing Approaches
Pain reprocessing approaches aim to reduce maladaptive fear responses and retrain the brain’s interpretation of pain signals. These approaches are based on the understanding that sensitised nervous systems can become excessively threat-focused.
The goal is not to deny the reality of symptoms, but to reduce the nervous system’s overprotective amplification response.
Trauma-Informed Care
Previous trauma, chronic stress and adverse life experiences can influence autonomic regulation, HPA-axis function and central sensitisation. Trauma-informed care recognises that these factors may shape nervous system responses without implying that symptoms are “all psychological”.
A supportive therapeutic relationship, validation and careful pacing are often particularly important in highly sensitised patients.
Key Clinical Message
Brain–gut behavioural therapies aim to reduce nervous system amplification and improve pain regulation rather than suggesting that symptoms are imaginary. In selected patients, they can meaningfully improve coping, autonomic regulation and functional recovery when combined with appropriate medical and physical treatment.
Interventional Pain Procedures
Most patients with visceral hypersensitivity do not require invasive procedures. The foundation of treatment remains careful diagnosis, education, neuromodulation, nervous system regulation, physical rehabilitation and appropriate management of underlying disease.
However, in selected patients with severe refractory pain, overlapping sympathetic dysfunction, pelvic pain syndromes, abdominal wall pain or focal nociceptive drivers, interventional pain procedures may sometimes play a useful role within a broader multidisciplinary treatment plan.
Importantly, interventions are rarely “standalone cures” for established central sensitisation. Their role is usually to reduce peripheral nociceptive input, interrupt pain amplification cycles, facilitate rehabilitation and improve quality of life.
When Interventions May Be Appropriate
Interventional procedures may be considered when symptoms remain severe despite appropriate conservative management, particularly where there is evidence of ongoing peripheral nociceptive input, pelvic floor dysfunction, sympathetically maintained pain or focal pain generators.
Careful patient selection is essential. The best outcomes are generally seen when interventions are integrated with physiotherapy, behavioural approaches, neuromodulation strategies and functional rehabilitation.
How Interventions May Fit Into a Multimodal Plan
Coeliac Plexus Block
The coeliac plexus is a major sympathetic plexus supplying upper abdominal organs including the pancreas, stomach, liver and proximal bowel. Coeliac plexus blocks are most strongly supported in pancreatic cancer pain and selected upper abdominal pain syndromes.
Their role in functional visceral hypersensitivity is much less established and careful patient selection is essential.
Splanchnic Nerve Block
Splanchnic nerve blocks target sympathetic pathways carrying visceral pain from the upper abdomen. They may occasionally be considered in selected refractory upper abdominal pain syndromes, particularly when sympathetically mediated pain is suspected.
Evidence in purely functional visceral hypersensitivity remains limited.
Superior Hypogastric Plexus Block
The superior hypogastric plexus carries sympathetic pain fibres from pelvic organs. Blocks targeting this region may occasionally help selected patients with chronic pelvic pain, endometriosis-related pain or sympathetically maintained pelvic pain.
These procedures are generally considered when significant pelvic pain persists despite conservative treatment.
Inferior Hypogastric Plexus Block
The inferior hypogastric plexus supplies deeper pelvic autonomic and visceral pathways. In selected patients, targeted intervention may help pelvic pain states involving visceral-autonomic amplification and pelvic organ sensitisation.
Evidence is evolving and these procedures are usually considered only within specialist pelvic pain practice.
Ganglion Impar Block
The ganglion impar is located near the coccyx and carries sympathetic input from the perineum, distal rectum, anus and coccygeal region. Ganglion impar blocks may help selected patients with coccydynia, perineal pain and pelvic sympathetic pain syndromes.
In carefully selected patients, pulsed radiofrequency techniques may also be considered.
Pudendal Nerve Interventions
Pudendal nerve interventions may occasionally be useful when pelvic pain involves clear pudendal distribution symptoms, pelvic floor hypertonicity or neuropathic-type perineal pain.
Approaches may include diagnostic nerve blocks or pulsed radiofrequency techniques in carefully selected patients. These interventions are usually considered alongside pelvic floor physiotherapy and broader management of central sensitisation.
Trigger Point Injections
Myofascial amplification frequently contributes to chronic abdominal and pelvic pain. Trigger point injections targeting abdominal wall muscles, pelvic floor muscles or associated myofascial structures may help reduce secondary muscle guarding and pain amplification.
These interventions are often most effective when combined with physiotherapy and rehabilitation rather than used in isolation.
Abdominal Wall Blocks
Abdominal wall pain syndromes such as anterior cutaneous nerve entrapment syndrome (ACNES) are frequently overlooked. Ultrasound-guided abdominal wall blocks may be both diagnostic and therapeutic in selected patients with focal abdominal wall tenderness and positive Carnett’s sign.
Identifying abdominal wall pain is important because it may mimic visceral disease while requiring a very different treatment approach.
Sympathetic Nervous System Modulation
Because visceral pain is closely linked to autonomic and sympathetic pathways, some interventions aim partly to modulate sympathetic nervous system activity rather than simply block nociceptive transmission.
This concept is particularly relevant in patients with sympathetically maintained pain, pelvic autonomic dysfunction, severe hyperalgesia or marked nervous system overactivation.
Evidence for interventions varies considerably depending on the underlying condition and procedure type.
| Procedure | Typical Indications | Typical Targets | Evidence Strength |
|---|---|---|---|
| Coeliac plexus block | Upper abdominal visceral pain, pancreatic pain | Coeliac plexus sympathetic pathways | Strongest evidence in pancreatic cancer pain |
| Splanchnic nerve block | Refractory upper abdominal pain | Thoracic splanchnic nerves | Moderate but condition-specific |
| Superior hypogastric plexus block | Chronic pelvic pain, endometriosis-related pain | Pelvic sympathetic plexus | Moderate specialist evidence |
| Inferior hypogastric plexus block | Complex pelvic visceral pain | Deep pelvic autonomic pathways | Emerging and specialist-based |
| Ganglion impar block | Perineal pain, coccydynia | Ganglion impar sympathetic pathways | Moderate evidence in selected patients |
| Pudendal nerve interventions | Perineal neuropathic pain and pelvic floor pain | Pudendal nerve pathways | Variable and patient-dependent |
| Trigger point injections | Myofascial abdominal or pelvic pain | Abdominal wall and pelvic floor muscles | Commonly used clinically |
| Abdominal wall blocks | ACNES and focal abdominal wall pain | Anterior cutaneous nerves and fascial planes | Good evidence in selected focal pain syndromes |
Important Clinical Perspective
Interventional procedures should not be viewed as universal solutions for visceral hypersensitivity or central sensitisation. The best outcomes are usually achieved when carefully selected interventions are integrated into a broader multidisciplinary treatment strategy addressing both peripheral and central pain mechanisms.
Pain Spa Expert Perspective
At Pain Spa, interventional procedures are used selectively within a broader multimodal framework rather than as isolated “quick fixes”. Careful assessment is performed to identify whether sympathetically maintained pain, pelvic floor dysfunction, abdominal wall pain or focal nociceptive drivers may be contributing to symptom amplification.
Where appropriate, advanced ultrasound-guided and fluoroscopy-guided procedures may be integrated alongside rehabilitation, neuromodulation strategies and nervous system regulation approaches to support functional recovery and reduce ongoing pain amplification.
A Stepwise Treatment Algorithm
Treatment of visceral hypersensitivity is rarely linear because patients often present with overlapping peripheral, autonomic, myofascial and central sensitisation mechanisms. The aim is usually gradual nervous system downregulation and functional recovery rather than a single “curative” intervention.
A stepwise approach helps avoid both undertreatment and unnecessary escalation to invasive therapies before simpler strategies have been optimised.
Stepwise Treatment Algorithm for Visceral Hypersensitivity
Conservative Measures
The first step is usually education, reassurance, treatment of underlying pathology, pacing, sleep optimisation and nervous system regulation. Lifestyle measures alone are rarely sufficient in severe sensitisation states, but they provide the foundation upon which all other treatments build.
Neuromodulators
Neuromodulator medications are often introduced early when pain amplification, sleep disturbance, hyperalgesia or autonomic dysregulation are prominent. Careful titration and realistic expectations are important because highly sensitised patients frequently experience medication sensitivity.
Psychological Therapies
Brain–gut behavioural therapies aim to reduce fear amplification, autonomic overactivation and maladaptive pain-processing cycles. These approaches work best when integrated with broader biological and physical treatment strategies rather than used in isolation.
Physical Therapy
Pelvic floor dysfunction, abdominal wall pain and myofascial amplification are common contributors to persistent visceral pain. Physical rehabilitation may therefore play an important role in restoring movement tolerance and reducing secondary muscular sensitisation.
Interventional Escalation
Targeted interventions may occasionally help selected patients with refractory focal pain generators, sympathetically maintained pain or pelvic autonomic amplification. Interventions should generally be used to support rehabilitation rather than as isolated “quick fixes”.
Complex Refractory Cases
Patients with severe long-standing sensitisation often require multidisciplinary care involving pain medicine, gastroenterology, pelvic health physiotherapy, psychology and rehabilitation strategies. Functional recovery may be gradual and typically involves reduction of nervous system reactivity rather than complete elimination of every symptom.
Key Clinical Message
The most effective treatment plans usually combine multiple approaches targeting both peripheral pain drivers and central sensitisation. Escalation to invasive procedures should be thoughtful, individualised and integrated into a broader functional rehabilitation strategy.
Frequently Asked Questions
“Are the symptoms real even if scans are normal?”
Yes. Visceral hypersensitivity and central sensitisation are recognised biological pain-processing disorders. Normal scans do not mean the symptoms are imagined. In many patients, the nervous system becomes overly sensitive, causing normal internal sensations to be interpreted as painful or threatening.
“Does this mean the pain is psychological?”
No. The pain is real and involves genuine biological changes in pain processing, neuroimmune signalling and autonomic regulation. Psychological stress can influence symptoms because the brain, gut and nervous system are closely connected — but this does not mean the pain is “all in the mind”.
“Can stress really affect the gut?”
Yes. Stress can influence gut motility, autonomic function, inflammation, mast cell activation and visceral sensitivity through the brain–gut axis. This is a biological nervous system response rather than a sign of weakness or imagined illness.
“Why do opioids make things worse?”
Long-term opioids can slow gut function, worsen constipation and increase nervous system sensitivity over time. Some patients develop opioid-induced hyperalgesia or narcotic bowel syndrome, where pain paradoxically becomes worse despite increasing opioid doses.
“Can visceral hypersensitivity improve?”
Yes, it can improve, although recovery is often gradual rather than immediate. Treatment usually focuses on reducing peripheral triggers, calming central sensitisation, improving sleep, restoring function, reducing fear-based amplification and supporting the brain–gut axis. Complete cure may not always be realistic, but meaningful improvement in pain, function and quality of life is often possible.
“Why do I have bladder and bowel symptoms together?”
The bowel, bladder, uterus, pelvic floor and lower abdominal structures share overlapping nerve pathways. Pain or inflammation in one organ can sensitise nearby organs through cross-organ sensitisation. This is why IBS-type symptoms, bladder pain, pelvic pain and endometriosis-related pain commonly overlap.
“Does visceral hypersensitivity mean nothing serious is going on?”
No. Red flag symptoms such as weight loss, bleeding, fever, anaemia, raised inflammatory markers, progressive neurological symptoms or a new change in bowel habit still require appropriate medical investigation. Visceral hypersensitivity should be diagnosed carefully, not assumed prematurely.
“Can surgery or treatment of the original problem fail to stop the pain?”
Yes. Sometimes the original condition may be treated successfully, but the nervous system remains sensitised. This can happen in endometriosis, diverticular disease, inflammatory bowel disease in remission, chronic pancreatitis and pelvic pain syndromes. Ongoing pain after technically successful treatment does not mean the pain is not real; it may mean the pain system itself now needs treatment.
“Are injections or procedures always needed?”
No. Many patients improve with education, neuromodulator medication, gut–brain therapies, pelvic floor treatment, dietary strategies, sleep improvement and gradual rehabilitation. Interventional procedures are considered only in selected patients where there is a clear target such as abdominal wall pain, pelvic floor trigger points, pudendal-type pain or sympathetically maintained pelvic pain.
“Can antihistamines or mast cell treatments help?”
They may help selected patients, particularly where mast cell–nerve interaction, food-related flares or neuroimmune activation appear relevant. However, antihistamines are not universal treatments for visceral hypersensitivity, and mast cell involvement does not automatically mean mast cell activation syndrome. These therapies should be considered as adjuncts within a broader treatment plan.
Key Clinical Message
Visceral hypersensitivity is real, biological and potentially treatable, but it requires careful diagnosis and a multimodal treatment plan. The goal is to reduce nervous system amplification, improve function and identify any treatable peripheral pain drivers without overlooking red flags or structural disease.
Pain Spa Expert Perspective & Treatments Offered
At Pain Spa, chronic abdominal, visceral and pelvic pain is approached through a modern neuroimmune and nervous-system-based framework rather than focusing purely on structural findings alone. Many patients presenting with persistent abdominal or pelvic pain have overlapping visceral hypersensitivity, pelvic floor dysfunction, autonomic dysregulation and central sensitisation.
Dr Krishna has extensive experience in the assessment and management of complex chronic pelvic pain, centrally mediated pain syndromes and refractory visceral pain presentations. Particular emphasis is placed on identifying pain–pathology mismatch, sympathetically maintained pain, myofascial amplification and overlapping central sensitisation features.
Where appropriate, advanced ultrasound-guided and fluoroscopy-guided procedures may be integrated into a broader multidisciplinary management plan. However, interventions are used selectively and are not presented as universal solutions for centrally sensitised pain states.
A trauma-informed and function-focused approach is considered particularly important in highly sensitised patients, especially where long-standing pain, autonomic hyperarousal, pelvic floor dysfunction or overlapping chronic pain syndromes are present.
Treatments Offered at Pain Spa
✔
Neuromodulator optimisation for visceral hypersensitivity and central sensitisation
✔
Ultrasound-guided abdominal wall injections and ACNES assessment
✔
Pelvic trigger point injections and myofascial pain treatment
✔
Sympathetic plexus procedures in selected refractory pelvic and visceral pain cases
✔
Ganglion impar procedures for selected perineal and coccygeal pain syndromes
✔
Pudendal nerve interventions in carefully selected patients
✔
Comprehensive chronic pelvic pain assessment
✔
Central sensitisation-focused and multidisciplinary pain management strategies
Clinical Philosophy at Pain Spa
Persistent visceral and pelvic pain is rarely explained by a single mechanism alone. At Pain Spa, management focuses on identifying the interaction between peripheral nociceptive drivers, pelvic floor dysfunction, autonomic dysregulation and central sensitisation, allowing treatment plans to be individualised rather than relying on a one-size-fits-all approach.
Key Clinical Take-Home Messages
1. Visceral hypersensitivity is a recognised biological pain-processing disorder involving abnormal amplification of sensory signals within the gut–brain axis and nervous system.
2. Normal scans or investigations do not mean symptoms are imaginary. Many patients have genuine nervous system sensitisation despite reassuring imaging.
3. Peripheral sensitisation, central sensitisation, autonomic dysregulation, neuroimmune activation and myofascial dysfunction often overlap.
4. Chronic abdominal, pelvic, bladder and bowel symptoms frequently coexist because of shared neural pathways and cross-organ sensitisation.
5. Ongoing pain after “successful” surgery or treatment does not necessarily mean the original diagnosis was wrong — the nervous system itself may remain sensitised.
6. Long-term opioid therapy may worsen visceral pain through opioid-induced hyperalgesia and worsening gut dysfunction.
7. Effective treatment usually requires a multimodal approach combining education, neuromodulators, behavioural therapies, rehabilitation and selected interventional procedures.
8. Mast cells, histamine pathways, microglia and neuroimmune signalling may contribute to symptom amplification in selected patients.
9. Psychological and brain–gut therapies are designed to reduce nervous system amplification and autonomic hyperarousal — not to suggest the pain is “all psychological”.
10. Red flag symptoms such as bleeding, weight loss, fever, progressive neurological symptoms or significant inflammatory markers should always prompt appropriate investigation.
Final Clinical Perspective
Visceral hypersensitivity sits at the intersection of gastroenterology, pain medicine, neuroimmunology, autonomic dysfunction and central sensitisation. Understanding this overlap is essential because many patients have historically been dismissed when structural investigations appear reassuring.
Modern management increasingly focuses on recognising the interaction between peripheral nociceptive input, neuroimmune activation, autonomic dysfunction and altered central pain processing. Although treatment can be challenging, carefully individualised multimodal management may significantly improve symptoms, function and quality of life in selected patients.
References
The following references represent major mechanistic papers, consensus guidance documents and key reviews relevant to visceral hypersensitivity, disorders of gut–brain interaction, central sensitisation, neuroimmune activation and chronic visceral pain.
Major Guidelines & Consensus Statements
- Drossman DA, Tack J, Ford AC, et al. Rome IV — Functional Gastrointestinal Disorders: Disorders of Gut–Brain Interaction. Gastroenterology. 2016;150(6):1257–1261.
- Lacy BE, Pimentel M, Brenner DM, et al. ACG Clinical Guideline: Management of Irritable Bowel Syndrome. American Journal of Gastroenterology. 2021;116(1):17–44.
- Sperber AD, Bangdiwala SI, Drossman DA, et al. Worldwide Prevalence and Burden of Functional Gastrointestinal Disorders, Results of Rome Foundation Global Study. Gastroenterology. 2021;160(1):99–114.
- Ford AC, Lacy BE, Talley NJ. Irritable Bowel Syndrome. New England Journal of Medicine. 2017;376:2566–2578.
- Camilleri M, Boeckxstaens G. Dietary and Pharmacological Treatment of Abdominal Pain in IBS. Gut. 2017;66(5):966–974.
- American Gastroenterological Association (AGA) Clinical Practice Updates on Disorders of Gut–Brain Interaction and Chronic Gastrointestinal Pain.
Visceral Hypersensitivity & Brain–Gut Mechanisms
- Mayer EA, Tillisch K, Gupta A. Gut/Brain Axis and the Microbiota. Journal of Clinical Investigation. 2015;125(3):926–938.
- Mayer EA, Labus JS, Tillisch K, et al. Towards a Systems View of IBS. Nature Reviews Gastroenterology & Hepatology. 2015;12(10):592–605.
- Simrén M, Barbara G, Flint HJ, et al. Intestinal Microbiota in Functional Bowel Disorders: A Rome Foundation Report. Gut. 2013;62(1):159–176.
- Grundy D, Al-Chaer ED, Aziz Q, et al. Fundamentals of Neurogastroenterology: Basic Science. Gastroenterology. 2006;130(5):1391–1411.
- Farmer AD, Aziz Q. Visceral Pain Hypersensitivity in Functional Gastrointestinal Disorders. British Medical Bulletin. 2013;107(1):123–136.
Central Sensitisation & Nociplastic Pain
- Woolf CJ. Central Sensitization: Implications for the Diagnosis and Treatment of Pain. Pain. 2011;152(3 Suppl):S2–S15.
- Nijs J, Van Houdenhove B, Oostendorp RA. Recognition of Central Sensitization in Patients with Musculoskeletal Pain. Pain Physician. 2010;13(3):E167–E183.
- Kosek E, Cohen M, Baron R, et al. Do We Need a Third Mechanistic Descriptor for Chronic Pain States? Pain. 2016;157(7):1382–1386.
- Fitzcharles MA, Cohen SP, Clauw DJ, et al. Nociplastic Pain: Towards an Understanding of Prevalent Pain Conditions. Lancet. 2021;397(10289):2098–2110.
Mast Cells, Histamine & Neuroimmune Activation
- Barbara G, Stanghellini V, De Giorgio R, et al. Activated Mast Cells in Proximity to Colonic Nerves Correlate with Abdominal Pain in IBS. Gastroenterology. 2004;126(3):693–702.
- Wouters MM, Vicario M, Santos J. The Role of Mast Cells in Functional GI Disorders. Gut. 2016;65(1):155–168.
- Aguilera-Lizarraga J, Florens MV, Viola MF, et al. Local Immune Response to Food Antigens Drives Meal-Induced Abdominal Pain. Nature. 2021;590(7844):151–156.
- Buhner S, Li Q, Vignali S, et al. Activation of Human Enteric Neurons by Supernatants of Colonic Biopsies from IBS Patients. Gastroenterology. 2009;137(4):1425–1434.
Microbiome & Gut–Brain Signalling
- Cryan JF, O’Riordan KJ, Cowan CSM, et al. The Microbiota–Gut–Brain Axis. Physiological Reviews. 2019;99(4):1877–2013.
- Dinan TG, Cryan JF. Gut Microbiota: A Missing Link in Psychiatry. World Psychiatry. 2020;19(1):111–112.
- Carabotti M, Scirocco A, Maselli MA, et al. The Gut–Brain Axis: Interactions Between Enteric Microbiota, Central and Enteric Nervous Systems. Annals of Gastroenterology. 2015;28(2):203–209.
Behavioural Therapies & Brain–Gut Interventions
- Lackner JM, Jaccard J, Krasner SS, et al. Self-Administered Cognitive Behavior Therapy for IBS. Clinical Gastroenterology and Hepatology. 2008;6(8):899–906.
- Palsson OS, Whitehead WE. Psychological Treatments in Functional Gastrointestinal Disorders. Clinical Gastroenterology and Hepatology. 2013;11(3):208–216.
- Keefer L, Keshavarzian A, Mutlu E. Reconsidering the Methodology of “Stress” Research in Gastrointestinal Illness. Journal of Crohn’s and Colitis. 2008;2(3):193–201.
Low Dose Naltrexone & Neuroimmune Modulation
- Younger J, Mackey S. Fibromyalgia Symptoms Are Reduced by Low-Dose Naltrexone: A Pilot Study. Pain Medicine. 2009;10(4):663–672.
- Younger J, Noor N, McCue R, et al. Low-Dose Naltrexone for the Treatment of Fibromyalgia. Arthritis & Rheumatology. 2013;65(2):529–538.
- Toljan K, Vrooman B. Low-Dose Naltrexone (LDN)—Review of Therapeutic Utilization. Medical Science. 2018;6(4):82.
Evidence Base Disclaimer
The understanding of visceral hypersensitivity, disorders of gut–brain interaction and neuroimmune pain mechanisms continues to evolve rapidly. Some treatments discussed in this article remain investigational or have variable evidence quality depending on the clinical context. Management decisions should always be individualised and guided by appropriate specialist assessment.