Ischial Bursitis
Bursitis is an inflammation or degeneration of the sac-like structures that protect the soft tissues from underlying bony prominences. Bursitis may result from a local insult or be a manifestation of a systemic disease. Examples of the latter include rheumatoid arthritis, tophaceous gout, and sepsis. Adjacent tenosynovitis and calcium apatite deposition disease commonly coexist.
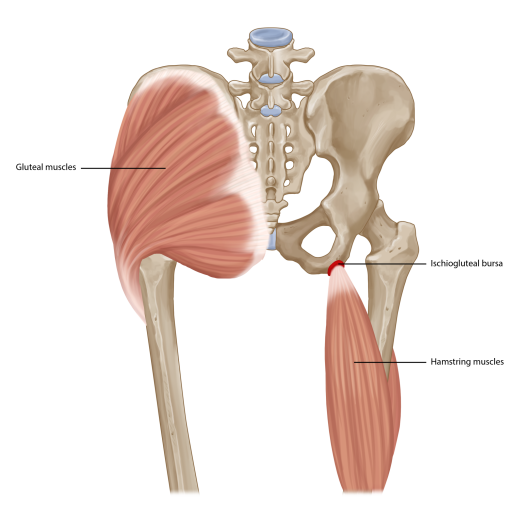
More than 140 bursae have been described in the human body. The clinically important bursae are the trochanteric, subdeltoid, ischiogluteal, pes anserine, iliopsoas, retrocalcaneal and olecranon bursae.