Costochondritis and Other Causes of Chest Wall Pain

Costochondritis and Lower Rib Pain Syndromes
Understanding Chest Wall Pain: Costochondritis, Slipping Rib Syndrome, Floating Rib Syndrome, and Twelfth Rib Syndrome
Introduction
Chest pain is one of the most alarming symptoms a person can experience. Many people understandably worry that pain in the chest must be coming from the heart or lungs.
In reality, a significant proportion of chest pain originates from the musculoskeletal structures of the chest wall rather than the heart or lungs. One of the most common causes is costochondritis, an inflammatory condition affecting the joints where the ribs connect to the sternum.
However, several other conditions involving the lower ribs can cause very similar symptoms, including slipping rib syndrome, floating rib syndrome, and twelfth rib syndrome. These conditions are frequently confused and can lead to prolonged diagnostic uncertainty.
Understanding the anatomy of the rib cage is essential for recognising the differences between these conditions and selecting the most appropriate treatment.
When to Seek Urgent Medical Help
Before assuming chest pain is due to a musculoskeletal cause, it is essential to rule out serious conditions first.
- Severe, crushing, or rapidly worsening chest pain
- Shortness of breath
- Sweating, nausea, dizziness, or collapse
- Pain radiating to the arm, jaw, or back
- Chest pain in someone with known heart disease or significant cardiac risk factors
Only once serious cardiac and pulmonary causes have been excluded should chest wall pain syndromes such as costochondritis be considered.
Anatomy of the Rib Cage
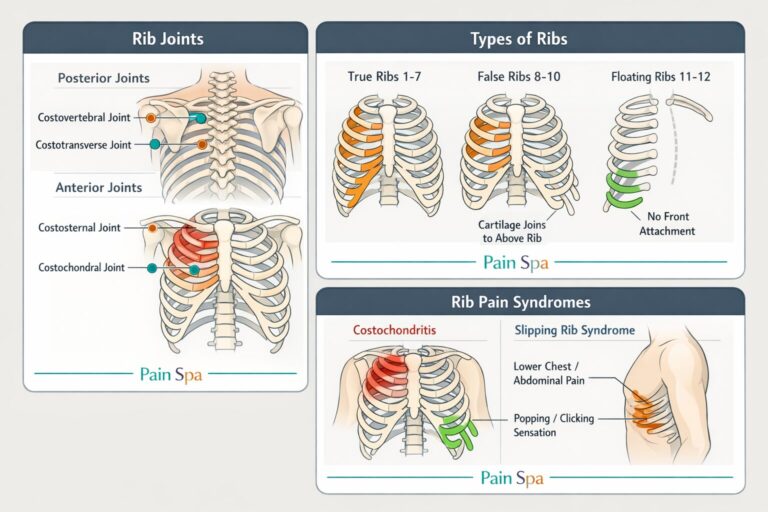
The rib cage consists of 12 pairs of ribs, which attach posteriorly to the thoracic spine and anteriorly to the sternum or costal cartilage.
True ribs (1–7) attach directly to the sternum via costal cartilage and are relatively stable.
False ribs (8–10) do not attach directly to the sternum. Instead, their cartilage joins the cartilage of the rib above, forming the costal margin. This arrangement makes these ribs more mobile and more vulnerable to instability syndromes such as slipping rib syndrome.
Floating ribs (11–12) do not attach to the sternum or to the costal cartilage in front. They attach only to the spine posteriorly. Because they lack anterior stabilisation, they are highly mobile and can produce flank or upper abdominal pain when irritated.
Anterior and Posterior Rib Joints
Each rib forms several joints.
Posterior joints include the costovertebral joint (rib with vertebral body) and the costotransverse joint (rib with transverse process). These joints allow rib movement during breathing.
Anterior joints include the costochondral joints (rib to cartilage) and the costosternal joints (cartilage to sternum). These are the anterior joints involved in costochondritis.
Causes and Risk Factors
Several factors can trigger chest wall pain syndromes.
Costochondritis may be associated with repetitive strain, heavy lifting, persistent coughing, viral respiratory infections, chest wall trauma, or inflammatory conditions such as arthritis.
Slipping rib syndrome is usually mechanical rather than purely inflammatory. It is often related to trauma, hypermobility, or weakening of the fibrous attachments between the false ribs.
Floating rib syndrome and twelfth rib syndrome may arise because the lower ribs are naturally more mobile. Trauma, poor posture, repetitive twisting movements, and irritation of nearby nerves can all contribute.
What Is Costochondritis?
Costochondritis is inflammation of the costochondral or costosternal joints located at the front of the chest where the ribs meet the sternum.
It most commonly affects ribs 2–5 and usually presents with localised tenderness over the affected joint or joints. This reproducible tenderness is one of the most important clinical clues.
The pain may be sharp, aching, or pressure-like and is often worsened by:
- Deep breathing
- Coughing or sneezing
- Upper body movement
- Exercise or lifting
Although the pain can be severe and frightening, costochondritis is usually benign and self-limiting once serious causes have been excluded.
Tietze Syndrome
Tietze syndrome is a rare inflammatory disorder of the costochondral joints that is often confused with costochondritis, but there are important differences.
Tietze syndrome often presents with acute pain and visible swelling over one costal cartilage. Treatment is broadly similar to costochondritis, including rest, analgesia, and anti-inflammatory medication. In selected cases, corticosteroid injections or, more rarely, a short course of oral steroids may be considered.
Differential Diagnosis of Chest Wall Pain
Chest wall pain can sometimes resemble symptoms caused by serious medical conditions. For this reason, clinicians must carefully exclude other potential causes before diagnosing costochondritis or other rib pain syndromes.
In clinical practice, careful history, examination, and appropriate investigations are used to exclude cardiac and pulmonary causes before diagnosing chest wall pain syndromes such as costochondritis.
Slipping Rib Syndrome
Slipping rib syndrome is a mechanical instability of the lower ribs, most commonly affecting ribs 8–10.
These are the false ribs, meaning they do not attach directly to the sternum. Instead, their cartilage joins the cartilage of the rib above. Because these ribs are connected by fibrous tissue rather than by a rigid direct sternal attachment, they can become hypermobile or subluxate.
The displaced rib tip may irritate the intercostal nerve, producing pain that is sharp, stabbing, and often movement-related.
Typical symptoms
- Lower chest or upper abdominal pain
- Sharp pain with twisting, bending, coughing, or sudden movement
- Clicking or popping sensation
- Pain radiating to the back or abdomen
- Symptoms that are often mechanical and positional rather than constant
Because the lower ribs are involved, slipping rib syndrome may present as upper abdominal or flank pain, which can easily be confused with gastrointestinal, renal, or spinal conditions.
Although pain from the lower false ribs may occasionally be loosely described by patients as “costochondritis,” classic costochondritis usually affects the upper anterior costochondral or costosternal joints, particularly ribs 2–5. The lower false ribs are much more commonly associated with slipping rib syndrome than with classic costochondritis.
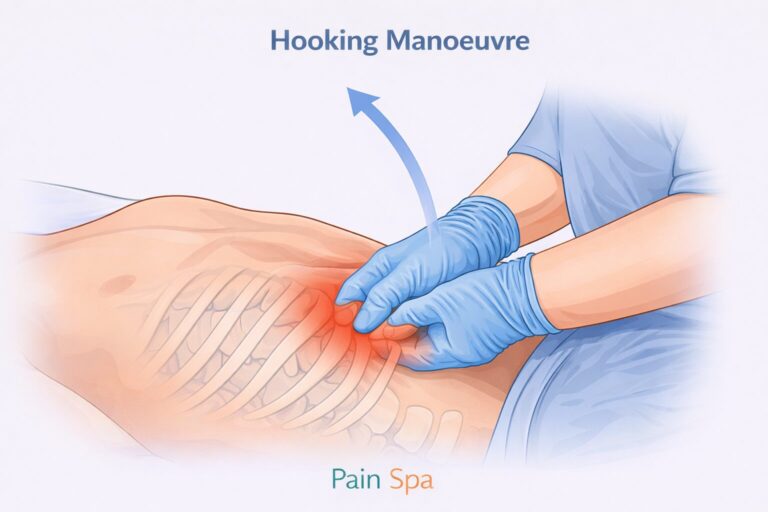
Diagnosis: The Hooking Manoeuvre
A useful clinical test for slipping rib syndrome and some lower rib pain syndromes is the hooking manoeuvre.
The clinician places fingers under the lower costal margin and then gently pulls the rib or costal margin anteriorly and superiorly. Reproduction of the patient’s familiar pain supports the diagnosis.
This manoeuvre can be very helpful clinically, although it may be uncomfortable. In selected cases, dynamic ultrasound can also demonstrate abnormal rib movement and help differentiate slipping rib syndrome from other causes of rib pain.
Floating Rib Syndrome
Floating ribs are ribs 11 and 12. Unlike the true and false ribs, they have no anterior attachment to the sternum or costal cartilage. They attach only posteriorly to the spine.
Because they are highly mobile, irritation or trauma can lead to pain in the:
- Lower chest
- Flank
- Upper abdomen
Symptoms arising from floating ribs can mimic renal, gastrointestinal, or spinal pathology. For this reason, these cases often undergo multiple investigations before the chest wall is recognised as the true source of the pain.
The term floating rib syndrome is sometimes used loosely, but it is helpful to distinguish general irritation of ribs 11–12 from the more specific entity of twelfth rib syndrome, in which the mobile twelfth rib irritates the subcostal nerve.
Twelfth Rib Syndrome
Twelfth rib syndrome occurs when the mobile twelfth rib irritates the subcostal nerve, producing pain in the lower chest, flank, loin, groin, or lower abdomen.
Typical symptoms include:
- Flank or loin pain
- Pain radiating to the groin or lower abdomen
- Pain worsened by walking, bending, twisting, or certain positions
- Tenderness around the lower rib margin
Because of its location, twelfth rib syndrome is often mistaken for kidney stones, abdominal pathology, or lumbar spine pain. The hooking manoeuvre may reproduce the familiar pain, and a diagnostic ultrasound-guided intercostal nerve block can be both confirmatory and therapeutic.
Differentiating Rib Pain Syndromes
Although these conditions can overlap, the pattern of pain, the ribs involved, and the underlying mechanism are often different. The table below provides a practical summary.
Conservative and Interventional Treatments for Persistent Chest Wall Pain
Most cases of costochondritis and lower rib pain improve with conservative management first. This may include:
- Rest and activity modification
- Simple analgesics or anti-inflammatory medication where appropriate
- Heat or ice depending on the stage and nature of symptoms
- Physiotherapy and movement modification
- Avoiding aggravating movements such as heavy lifting or repeated twisting
However, some patients develop persistent or chronic chest wall pain. In these cases, interventional pain treatments may provide significant relief once serious pathology has been excluded.
Ultrasound-Guided Costochondral or Costosternal Joint Injections
Ultrasound guidance allows precise treatment of the inflamed joint while avoiding nearby sensitive structures. These injections typically include a local anaesthetic and a corticosteroid.
Potential benefits include:
- Reduction in inflammation
- Pain relief
- Improved comfort with breathing, movement, and daily activity
Intercostal Nerve Blocks
The intercostal nerves supply the rib cage and the costochondral region. When irritated, they can produce severe, persistent chest wall pain.
An ultrasound-guided intercostal nerve block can be used both diagnostically and therapeutically. If the patient gets clear temporary relief, this helps confirm that the nerve is a major pain generator.
These blocks are particularly useful in:
- Slipping rib syndrome
- Twelfth rib syndrome
- Chronic costochondral pain with a neuropathic component
Pulsed Radiofrequency Treatment
If nerve blocks provide good but short-lived relief, pulsed radiofrequency (PRF) treatment may be considered. PRF delivers controlled electrical pulses to the nerve without destroying it, aiming to reduce abnormal pain signalling.
Potential benefits may include:
- Longer-lasting pain relief in selected patients
- Minimal tissue damage
- Reduced need for repeated injections
PRF is typically considered after a successful diagnostic block has shown that the relevant nerve is contributing to the pain.
Regenerative Treatments
In selected patients with persistent rib instability, ligament strain, or chronic soft-tissue irritation, regenerative treatments may be considered.
Platelet-Rich Plasma (PRP) uses the patient’s own platelets to promote healing of irritated cartilage and ligaments.
Prolotherapy is designed to stimulate tissue repair and strengthen weakened ligamentous structures.
These treatments are generally considered as part of a broader rehabilitation strategy and are usually most relevant when there is a suspected mechanical or ligamentous component to ongoing symptoms.
Surgical Options
In severe or refractory slipping rib syndrome, surgical options such as resection or stabilisation may occasionally be considered. These are usually reserved for carefully selected cases when conservative and interventional options have not provided adequate relief.
Expert Care at Pain Spa
At Pain Spa Bristol, Dr Krishna has extensive experience diagnosing and treating complex chest wall pain conditions, including costochondritis, slipping rib syndrome, floating rib pain, and twelfth rib syndrome.
Using advanced ultrasound-guided techniques, we aim to identify the primary pain generator as accurately as possible, whether that is the joint, the intercostal nerve, or the surrounding soft tissues.
Available treatments may include:
- Ultrasound-guided costochondral or costosternal joint injections
- Intercostal nerve blocks
- Pulsed radiofrequency treatment
- PRP therapy
- Prolotherapy
This mechanism-based approach allows many patients with persistent chest wall pain to achieve meaningful improvement in pain, function, and quality of life.
Key Take-Home Messages
- Costochondritis is a common cause of anterior chest wall pain once serious pathology has been excluded.
- Lower rib pain may instead be due to slipping rib syndrome, floating rib syndrome, or twelfth rib syndrome, which often mimic abdominal, renal, or spinal conditions.
- Careful clinical examination, including the hooking manoeuvre where appropriate, is important in differentiating these conditions.
- Most cases improve with conservative treatment, but ultrasound-guided injections, intercostal nerve blocks, and pulsed radiofrequency can be very helpful in persistent cases.
- Accurate diagnosis is essential because not all chest wall pain is the same, and treatment should be tailored to the underlying pain mechanism.
If you suffer from costochondritis or chest wall pain and would like a specialist assessment, please contact Pain Spa at clinic@painspa.co.uk or visit www.painspa.co.uk for further information. A structured, mechanism-based plan can significantly improve outcomes.