Discogenic Low Back Pain: Understanding the Cause and the Treatments That Can Help

Discogenic Low Back Pain
A Comprehensive Clinical Review
Pain Spa Clinical Education Series
Introduction
Discogenic low back pain is one of the most common yet often under-recognised causes of chronic axial low back pain. It arises from structural and biochemical changes within the intervertebral disc and can lead to significant functional impairment and reduced quality of life.
A central challenge in clinical practice is the poor correlation between imaging and symptoms. Degenerative disc changes are extremely common, particularly with advancing age, and are frequently seen in individuals without pain. The presence of disc degeneration on MRI, therefore, does not in itself establish a diagnosis.
Discogenic pain represents the subset in which the disc has become an active pain generator, typically through a combination of structural disruption, inflammation, and altered innervation. Accurate diagnosis requires careful integration of clinical features, imaging findings, and exclusion of other pain sources.
At Pain Spa, emphasis is placed on a mechanism-based approach, combining clinical assessment with targeted interventions. In selected patients, lumbar epidural injections and L2 dorsal root ganglion-targeted treatments form key components of the treatment pathway.
Epidemiology and Risk Factors
Discogenic low back pain most commonly affects individuals in the 30–60 year age group, often during peak working years. While disc degeneration becomes increasingly prevalent with age, the development of symptomatic pain reflects a combination of biological, mechanical, and psychosocial factors.
Genetic predisposition plays a significant role, with a substantial proportion of disc degeneration variance shown to be heritable. Mechanical loading, including repetitive bending, lifting, and prolonged sitting, increases intradiscal pressure and contributes to disc stress over time.
Lifestyle factors such as obesity and smoking may further accelerate degenerative change, while psychosocial factors, including fear avoidance, stress, and reduced activity, are strongly associated with persistence of symptoms and disability.
Discogenic pain should therefore be understood as a multifactorial condition rather than a purely structural abnormality.
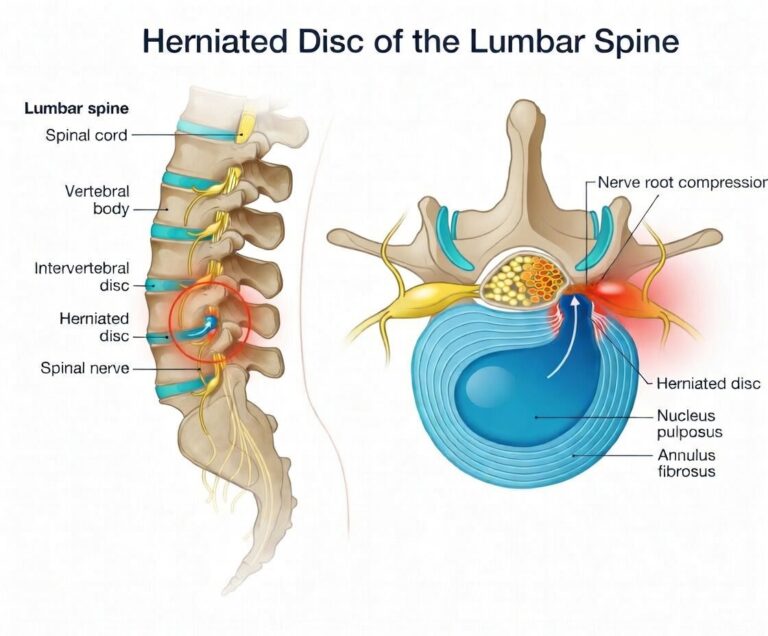
Pathophysiology
The normal intervertebral disc is largely avascular and only sparsely innervated, with nociceptive fibres confined to the outer annulus. During degeneration, progressive structural disruption leads to loss of hydration, reduced load distribution, and increased mechanical stress.
Annular fissures allow inflammatory mediators to extend beyond their usual boundaries, sensitising nociceptors and contributing to persistent pain. Over time, there is ingrowth of nerve fibres into deeper regions of the disc, creating a structural basis for ongoing nociceptive signalling.
In some patients, repeated nociceptive input leads to central sensitisation, amplifying pain beyond the original structural abnormality. In parallel, the vertebral endplate may become involved, resulting in a degree of vertebrogenic overlap, particularly when Modic changes are present.
This combination of structural, inflammatory, and neurophysiological change explains why discogenic pain can be both persistent and difficult to treat.
Clinical Presentation
Discogenic low back pain typically presents as central or paramedian axial pain, often described as deep, aching, or pressure-like.
A defining feature is its relationship to mechanical loading. Symptoms are commonly worsened by sitting and forward flexion, aggravated by prolonged posture or driving, and improved by unloading or lying down.
Pain may refer into the buttocks or upper thighs but does not usually follow a dermatomal distribution and is not typically associated with objective neurological deficit.
This pattern of load-sensitive axial pain, in the absence of radiculopathy, is strongly suggestive of a discogenic source when supported by imaging.
Diagnosis
MRI remains the investigation of choice and provides important structural information. Findings such as disc degeneration, annular fissures, high-intensity zones, and Modic changes may support the diagnosis when aligned with the clinical picture.
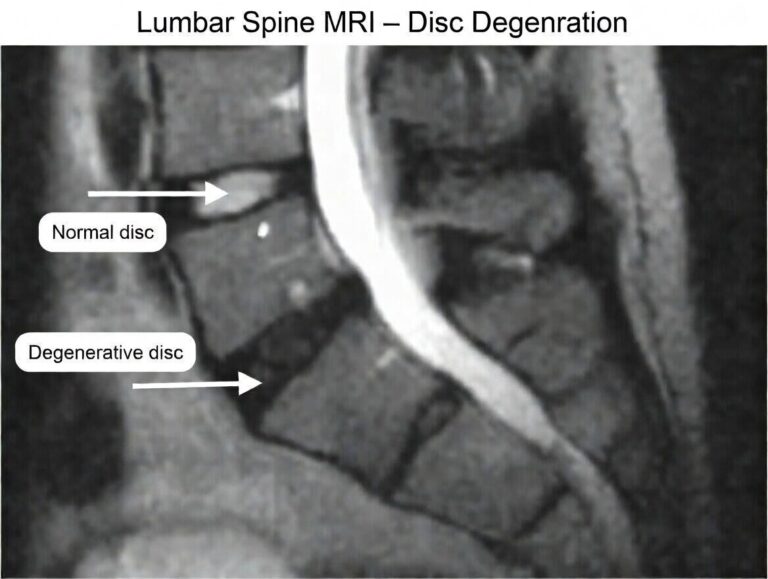
Among these, Modic Type 1 changes and annular fissures are particularly relevant indicators of symptomatic pathology. However, it is essential to recognise that degenerative changes are common and frequently incidental. Diagnosis therefore depends on careful clinical-radiological correlation, with exclusion of other pain generators such as facet joints, sacroiliac joints, and nerve root irritation.
Provocative discography has historically been regarded as the reference diagnostic test for confirming discogenic pain when uncertainty remains and when the result would meaningfully alter management. The procedure involves fluoroscopically guided injection of contrast into the suspected disc to determine whether this reproduces the patient’s familiar pain, usually alongside assessment of disc morphology and comparison with at least one control level.
However, the use of discography remains controversial, and the jury is still out. Concerns include false-positive responses, particularly in patients with heightened pain sensitivity or psychological distress, as well as the possibility of accelerating disc degeneration after needle penetration. Its ability to predict outcomes following surgery or other interventions is also variable.
For these reasons, discography is not used routinely and is best reserved for carefully selected cases in which clinical assessment and imaging remain inconclusive, particularly when an invasive or surgical treatment is being considered. Even then, findings should be interpreted within the broader clinical context rather than in isolation.
Conservative Management
Conservative treatment remains the foundation of management and should usually be optimised before interventional options are considered. A structured rehabilitation programme focusing on core stability, graded strengthening, mobility, and aerobic conditioning is essential.
Patients should be encouraged to remain active and avoid prolonged inactivity, which tends to worsen deconditioning and long-term disability. Physiotherapy, pacing, activity modification, and appropriate pain education all have an important role.
Psychological and behavioural factors also matter. Fear avoidance, reduced confidence in movement, poor sleep, and chronic stress can all contribute to persistent symptoms, so a broader multidisciplinary approach is often helpful in more complex cases.
Medication may provide symptomatic relief in selected patients, particularly where it helps facilitate engagement with rehabilitation, but it should be used judiciously and not seen as the sole answer.
Lumbar Epidural Injections
Lumbar epidural injections remain a key component of interventional pain management. While the strongest evidence supports their use in radicular pain, they also have a valuable role in selected patients with discogenic low back pain, particularly where inflammation is contributing to symptom persistence.
The mechanism of action is primarily anti-inflammatory, reducing the activity of mediators associated with annular disruption and disc degeneration. Local anaesthetic provides short-term interruption of nociceptive signalling, while the injectate volume itself may contribute to mechanical and biochemical modulation within the epidural space.
It is important to set realistic expectations. In discogenic pain, epidural injections typically provide short- to medium-term relief rather than permanent resolution. Their clinical value lies in reducing pain sufficiently to allow progression with rehabilitation and functional recovery.
The interlaminar approach is generally most appropriate for axial or bilateral symptoms, allowing broader distribution within the epidural space. The transforaminal approach offers more targeted delivery when there is a clear symptomatic level or lateralised component. Caudal epidural injections provide a simpler and often safer alternative in selected cases, although they are less anatomically specific.
At Pain Spa, epidural injections are used in a targeted and pragmatic manner, guided by clinical presentation and imaging. They are not viewed as standalone solutions, but as part of a structured treatment strategy in which response is carefully assessed and further management adapted accordingly.
L2 Dorsal Root Ganglion Block and Pulsed Radiofrequency
The L2 dorsal root ganglion represents a key target in the management of discogenic low back pain due to the convergence of disc afferent pathways at this level.
Nociceptive signals from multiple lumbar discs may travel via sympathetic pathways and converge at the L2 dorsal root ganglion. This provides a strong anatomical basis for targeting L2, even when the primary disc pathology lies at lower lumbar levels.
An L2 dorsal root ganglion block can be used diagnostically, with meaningful reduction in familiar pain supporting a discogenic mechanism. While not definitive in isolation, it provides useful information when interpreted alongside the overall clinical picture, imaging findings, and exclusion of other pain sources.
From a therapeutic perspective, some patients also experience significant improvement following L2 blockade, reflecting the importance of this pathway in pain transmission. Where benefit is present but not sustained, pulsed radiofrequency may be considered. This delivers controlled electrical energy to modulate pain signalling without causing thermal destruction of neural tissue, offering a favourable safety profile.
While high-quality direct evidence in pure discogenic pain remains limited, the combination of anatomical rationale, clinical experience, and observed patient outcomes supports its use in carefully selected patients. At Pain Spa, L2 dorsal root ganglion-targeted treatment is used as part of a mechanism-based approach, particularly where epidural injections provide incomplete or short-lived benefit.
Intradiscal Procedures
Intradiscal procedures aim to treat the disc directly and are used in more selected cases. Techniques such as intradiscal biacuplasty have shown benefit in appropriately selected patients with contained disc pathology.
Other procedures, including intradiscal electrothermal therapy and nucleoplasty, have more limited and inconsistent evidence and are less commonly used in modern practice.
A key consideration is the potential for disc injury associated with direct intervention. For this reason, intradiscal procedures are reserved for carefully selected patients and are not first-line treatments.
Basivertebral Nerve Ablation (Vertebrogenic Pain)
Basivertebral nerve ablation is a well-supported treatment for vertebrogenic pain associated with Modic changes. It targets nociceptive input from the vertebral endplate and can provide durable improvement in appropriately selected patients.
This is particularly relevant given the overlap between discogenic and vertebrogenic pain, and highlights the importance of careful imaging interpretation in guiding treatment.
Dorsal Root Ganglion Stimulation
Dorsal root ganglion stimulation is an advanced neuromodulation technique that provides targeted electrical modulation of specific dorsal root ganglia.
In discogenic pain, targeting the L2 dorsal root ganglion is of particular interest, and early studies suggest meaningful improvements in selected patients. However, this is a more invasive option and is typically reserved for refractory cases.
Spinal Cord Stimulation
Spinal cord stimulation has an established role in chronic pain but has historically been less effective for isolated axial low back pain. Newer technologies have improved its applicability in this setting.
It may be considered in patients with persistent symptoms despite other treatments, but remains a later-stage intervention requiring careful patient selection.
Regenerative and Biological Therapies
Regenerative therapies aim to address the underlying disc pathology rather than simply modulating pain.
Intradiscal platelet-rich plasma has shown promising early results, although variability in technique and limited high-quality evidence mean that it remains an evolving treatment.
Stem cell therapies and other biological approaches are under investigation but are not yet part of routine clinical practice. These treatments should therefore be viewed as promising but not yet established.
Surgical Management
Surgery is reserved for selected patients with severe, persistent symptoms who have not responded to conservative and interventional treatment.
Options include spinal fusion and disc replacement. Outcomes are variable, and careful patient selection is essential.
Integrated Treatment Approach
Management should follow a structured progression, beginning with conservative care and advancing through targeted interventional treatments based on clinical response and imaging findings.
Epidural injections and L2 dorsal root ganglion-based approaches form key intermediate steps, with more advanced interventions considered where necessary.
Treatments Offered at Pain Spa
At Pain Spa, treatment is tailored to the individual patient, based on careful clinical assessment, imaging correlation, and response to prior therapies. The focus is on precision, safety, and appropriate patient selection rather than a one-size-fits-all approach.
| Treatment option | Availability at Pain Spa | Comment |
|---|---|---|
| Lumbar epidural injection under image guidance | ✓ Offered | Used in selected patients to reduce inflammation, improve pain control, and facilitate rehabilitation. |
| Caudal epidural injection | ✓ Offered | A useful option in selected cases where broader epidural spread is appropriate. |
| L2 dorsal root ganglion block | ✓ Offered | Used diagnostically and therapeutically where discogenic pain is strongly suspected. |
| L2 dorsal root ganglion pulsed radiofrequency | ✓ Offered | A minimally invasive neuromodulatory option in carefully selected patients. |
All procedures at Pain Spa are performed with a strong emphasis on image guidance, anatomical precision, and careful patient selection, ensuring that treatment is aligned with the underlying pain mechanism.
Procedures Not Currently Offered at Pain Spa
It is equally important to be clear about the procedures that are discussed in the wider evidence base but are not currently offered through Pain Spa for discogenic low back pain.
| Procedure | Availability at Pain Spa | Comment |
|---|---|---|
| Provocative discography | ✕ Not offered | Its role remains controversial and it is generally reserved for highly selected diagnostic situations. |
| Intradiscal PRP for disc pain | ✕ Not offered | An evolving regenerative option, but not currently part of the Pain Spa treatment pathway for discogenic pain. |
| Spinal cord stimulation | ✕ Not offered | A later-stage neuromodulation option that sits outside the current Pain Spa offering for discogenic low back pain. Offered through NHS Pain Clinic in Bristol |
| Intradiscal biacuplasty | ✕ Not offered | Discussed in the treatment landscape but not currently offered through Pain Spa. |
Key Clinical Pearls
Disc degeneration does not equate to pain, and diagnosis requires careful clinical correlation. Discogenic pain is typically load-sensitive and worsened by sitting and flexion.
Epidural injections can provide meaningful benefit in selected patients, particularly when used to support rehabilitation. L2 dorsal root ganglion-targeted treatment offers a mechanism-based approach aligned with current understanding of disc innervation pathways.
Effective management requires a multimodal and individualised approach, with interventions used judiciously and guided by response.
Conclusion
Discogenic low back pain is a complex condition requiring a structured and evidence-informed approach. While many patients improve with conservative care, interventional treatments play an important role in selected cases.
At Pain Spa, particular emphasis is placed on lumbar epidural injections and L2 dorsal root ganglion-targeted treatments, which reflect current understanding of discogenic pain pathways.
The key to successful management lies in selecting the right patient for the right treatment within a carefully planned and individualised strategy.
Disclaimer
This article is intended for educational purposes only and should not replace individual clinical assessment or judgement. Treatment decisions should always be based on full history, examination, imaging review, and discussion of appropriate options for the individual patient.