Migraine Headaches: A Comprehensive Guide to Diagnosis, Evidence-Based Treatment, and Advanced Interventional Options

Migraine Headaches: Evidence-Based Diagnosis, Medical Management and Advanced Interventional Treatments
Migraine is one of the most common and disabling neurological disorders worldwide. It affects around 12–15% of the population, is markedly more common in women, and is especially prevalent during the most productive adult years. It remains a major cause of disability, reduced quality of life, lost work capacity, and repeated healthcare use. Migraine with aura also carries additional clinical importance because of its association with ischaemic stroke risk, particularly in women who smoke or use combined hormonal contraception. Despite this, migraine is still underdiagnosed and undertreated, and many patients receive fragmented care focused only on pain relief rather than a structured long-term management plan.
Migraine care has changed substantially in recent years. It now requires accurate diagnosis, thoughtful differentiation from other headache disorders, evidence-based acute treatment, appropriate use of prevention, integration of behavioural and lifestyle strategies, selective use of neuromodulation devices, and, in suitable patients, targeted interventional procedures such as Botox, greater occipital nerve blocks, pulsed radiofrequency, and other cranial nerve blocks. At Pain Spa, migraine is approached in exactly this comprehensive, layered, and individualised way.
Understanding Migraine: Pathophysiology
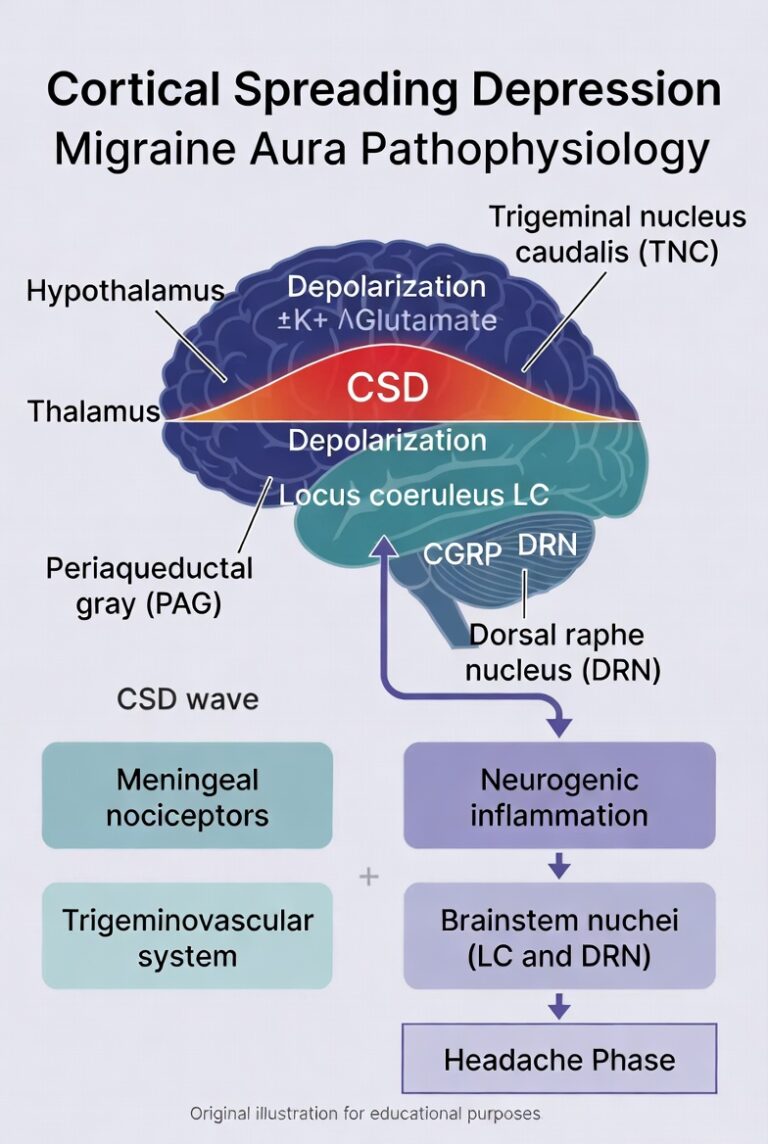
Migraine is no longer regarded as simply a vascular headache. It is now understood as a complex neurological disorder involving dysfunction of central pain-modulating pathways, activation of the trigeminovascular system, cortical hyperexcitability, and progressive sensitisation of nociceptive networks. The trigeminal nerve, particularly through its ophthalmic division, innervates the meninges and meningeal blood vessels. When activated, it releases vasoactive neuropeptides, especially calcitonin gene-related peptide (CGRP), along with substance P and neurokinin A. CGRP is central to migraine pathophysiology: it promotes meningeal vasodilation, sensitises peripheral trigeminal afferents, and amplifies nociceptive signalling. This is the basis for the major therapeutic advances represented by gepants and CGRP monoclonal antibodies.

Migraine aura is thought to reflect cortical spreading depression, a slowly propagating wave of neuronal and glial depolarisation followed by suppression of activity across the cortex. Repeated trigeminal activation may lead first to peripheral sensitisation and then to central sensitisation within the trigeminal nucleus caudalis and higher-order thalamic pathways. This helps explain allodynia, increased attack severity, and the transformation from episodic to chronic migraine. Hypothalamic and brainstem dysfunction also contributes to prodromal symptoms such as yawning, food cravings, neck stiffness, fatigue, and mood change. A proper understanding of these mechanisms is important because modern migraine treatments target different points along this pathway rather than simply masking pain.
Diagnosis of Migraine
Migraine is a clinical diagnosis based on history and examination. There is no routine diagnostic biomarker. Most patients with migraine have a normal neurological examination, and the diagnosis depends on correctly applying the International Classification of Headache Disorders, 3rd edition (ICHD-3) criteria.
ICHD-3 Diagnostic Criteria
Migraine without aura
This is the most common form of migraine. Diagnosis requires at least five attacks fulfilling the following:
| Criterion | Requirement |
|---|---|
| Attack duration | 4–72 hours untreated or unsuccessfully treated |
| Pain characteristics | At least 2 of the following: unilateral location; pulsating quality; moderate or severe intensity; aggravation by routine physical activity or causing avoidance of activity |
| Associated symptoms | At least 1 of the following: nausea and/or vomiting; photophobia and phonophobia |
| Alternative explanation | Not better accounted for by another ICHD-3 diagnosis |
Migraine with aura
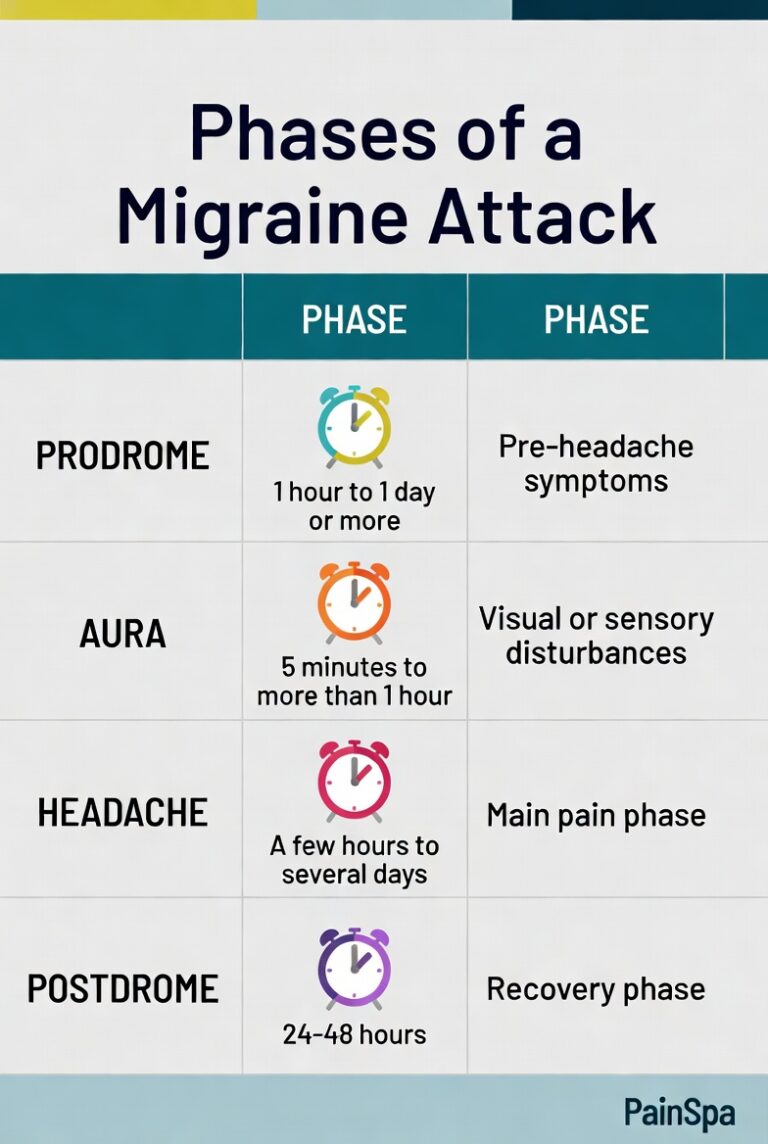
This requires at least two attacks with fully reversible aura symptoms. These may be visual, sensory, speech/language, motor, brainstem, or retinal. Symptoms usually spread gradually over at least 5 minutes, last 5–60 minutes, and are followed by headache within 60 minutes. Visual aura is the most common pattern and may present as scintillating scotoma or fortification spectra.
Chronic migraine
Chronic migraine is defined as headache occurring on 15 or more days per month for more than 3 months, with migraine features on at least 8 days per month. This distinction matters greatly because it changes the treatment pathway, especially in relation to Botox, CGRP-targeted prevention, and interventional strategies.
Probable migraine
Patients who meet all but one of the usual criteria may be classified as having probable migraine. These patients are often mislabelled as having tension-type headache, but the underlying biology and treatment principles are similar. The POUND mnemonic — Pulsating, duration 4–72 hOurs, Unilateral, Nausea, Disabling — can be useful in clinical practice.
Key clinical features of migraine
| Feature | Typical migraine characteristic |
|---|---|
| Pain quality | Pulsating or throbbing |
| Location | Often unilateral, though bilateral pain is not uncommon, especially in chronic migraine |
| Severity | Moderate to severe; interferes with function |
| Associated symptoms | Nausea, vomiting, photophobia, phonophobia |
| Behaviour | Worsened by movement; patient often prefers to lie still in a dark quiet room |
| Duration | 4–72 hours untreated |
| Premonitory symptoms | Yawning, food cravings, neck stiffness, fatigue, mood change |
| Postdrome | Cognitive fog, fatigue, scalp tenderness |
A full migraine attack may progress through four phases: prodrome, aura, headache, and postdrome. Not every patient experiences all phases, but recognising them is clinically helpful because it encourages earlier treatment and improves diagnostic confidence.
Role of neuroimaging
Neuroimaging is not routinely required in patients with stable, typical migraine symptoms and a normal neurological examination. MRI is preferred over CT where imaging is needed. Imaging should be considered in first or worst headache, thunderclap onset, unusual or prolonged aura, hemiplegic migraine, migraine with brainstem aura, progressively worsening pattern, side-locked headache, new onset after age 50, headache associated with systemic illness, exertional headache, postural headache, papilloedema, or focal neurological signs.
Red flags
Features suggesting secondary headache include thunderclap onset, fever, neck stiffness, immunosuppression, cancer, papilloedema, pregnancy, neurological deficit, recent trauma, new onset after age 50, and progressive worsening. Headache that changes significantly in pattern or becomes resistant to usual migraine treatment also deserves reassessment.
Differential Diagnosis
Distinguishing migraine from other primary headache disorders is essential because management differs significantly.
Migraine vs tension-type headache
Tension-type headache is usually bilateral, pressing or tightening rather than pulsating, mild to moderate rather than severe, not aggravated by routine physical activity, and usually lacks nausea or both photophobia and phonophobia. Migraine is more disabling, more likely to be pulsating, associated with nausea, and worsened by movement.
Migraine vs trigeminal autonomic cephalalgias
Cluster headache and related trigeminal autonomic cephalalgias are shorter, often more severe, and associated with prominent ipsilateral autonomic symptoms such as tearing, rhinorrhoea, conjunctival injection, ptosis, or miosis. Patients with migraine tend to keep still; patients with cluster headache are often restless and pacing. Duration is particularly useful diagnostically: migraine usually lasts 4–72 hours, whereas cluster headache typically lasts 15–180 minutes. Paroxysmal hemicrania and hemicrania continua show an absolute response to indomethacin, which is diagnostically important.
Migraine vs new daily persistent headache
New daily persistent headache is distinguished by a clearly remembered onset: the patient can often identify the exact day the daily continuous headache began. Chronic migraine usually evolves gradually from episodic migraine over time.
Acute Treatment of Migraine
The goals of acute treatment are to relieve pain quickly, restore function, reduce associated symptoms such as nausea and photophobia, minimise recurrence, and avoid unnecessary escalation into frequent medication use. Current evidence supports a stratified approach, selecting therapy according to attack severity, nausea/vomiting, comorbidities, and prior response. The American College of Physicians recommends NSAIDs or acetaminophen first for milder attacks, with triptan-based therapy for more severe or disabling migraine. Combination therapy with a triptan and an NSAID has particularly strong evidence.
General principles of acute treatment
Acute medication works best when taken early in the attack, before the pain becomes severe and before central sensitisation is firmly established. Adequate dose matters. Route matters too: oral treatment is appropriate for many attacks, but nasal or injectable options become important when nausea, vomiting, or very rapid escalation are prominent. Acute therapy should also be monitored carefully so that treatment itself does not become part of the problem through repeated escalation.
Evidence-based acute drug options
| Drug class | Medication | Dose | Maximum daily dose | Key points |
|---|---|---|---|---|
| Analgesic | Paracetamol | 1000 mg | 4000 mg | Useful in milder attacks; less effective than NSAIDs for moderate–severe migraine |
| NSAID | Ibuprofen | 400–600 mg | 2400 mg | Good first-line option for mild–moderate migraine |
| NSAID | Naproxen | 500–750 mg | 1250 mg | Longer acting; useful where recurrence is a problem |
| NSAID | Diclofenac | 50–100 mg | 150 mg | Rapid onset; useful in moderate attacks |
| NSAID | Aspirin | 500–1000 mg | 4000 mg | Can be effective, especially with antiemetic support |
| Triptan | Sumatriptan oral | 50–100 mg | 200 mg | Standard migraine-specific option |
| Triptan | Sumatriptan subcutaneous | 6 mg | 12 mg | Fastest onset; very useful in severe attacks or marked nausea |
| Triptan | Sumatriptan nasal | 20 mg | 40 mg | Useful non-oral option |
| Triptan | Rizatriptan | 10 mg | 30 mg | Fast acting; reduce dose if taking propranolol |
| Triptan | Eletriptan | 40 mg | 80 mg | High efficacy; watch CYP3A4 interactions |
| Triptan | Zolmitriptan | 5 mg | 10 mg | Oral or nasal formulations available |
| Triptan | Naratriptan | 2.5 mg | 5 mg | Slower onset, lower recurrence |
| Triptan | Frovatriptan | 2.5 mg | 7.5 mg | Long half-life; useful in menstrual migraine |
| Combination | Sumatriptan + naproxen | 85/500 mg | 2 tablets | Greatest net benefit in ACP guidance |
| Gepant | Ubrogepant | 50–100 mg | 200 mg | No vasoconstriction; useful in cardiovascular contraindications |
| Gepant | Rimegepant ODT | 75 mg | 75 mg | Acute and preventive indications |
| Gepant | Zavegepant nasal | 10 mg | 10 mg | Rapid non-oral option |
| Ditan | Lasmiditan | 50–200 mg | 200 mg | Non-vasoconstrictive but sedating; no driving for 8 hours |
| Antiemetic | Metoclopramide | 10 mg | 30 mg | Helps nausea and may improve overall acute response |
| Antiemetic | Prochlorperazine | 10 mg | 40 mg | Particularly useful in urgent care / ED settings |
How to choose acute treatment
For mild to moderate migraine, NSAIDs such as ibuprofen, naproxen, diclofenac, or aspirin remain evidence-based first-line options. Paracetamol is less effective overall but can still be helpful in mild attacks or when NSAIDs are unsuitable. For moderate to severe migraine, or attacks that consistently disrupt function, triptans remain the main migraine-specific acute therapy. Patients who only partly respond to simple analgesics often do best with escalation to a triptan or a triptan–NSAID combination, especially sumatriptan plus naproxen.
When triptans are unsuitable
Triptans are contraindicated in ischaemic heart disease, uncontrolled hypertension, prior stroke or TIA, and significant peripheral vascular disease. This is where gepants and lasmiditan are especially important. They do not cause vasoconstriction and provide migraine-specific alternatives for patients who cannot safely use triptans. Gepants are particularly attractive in patients with cardiovascular disease, triptan intolerance, or insufficient response to triptans. Lasmiditan is also non-vasoconstrictive, but its sedative profile makes it less convenient for some patients.
Status migrainosus and urgent treatment
Prolonged or refractory attacks may require escalation. In emergency settings, evidence-based parenteral options include prochlorperazine, metoclopramide, valproate, ketorolac, and droperidol. Corticosteroids such as dexamethasone may be used as adjuncts to reduce recurrence. Greater occipital nerve block has also emerged as an important acute interventional option in refractory migraine and status migrainosus.
What is not recommended
Opioids and barbiturate-containing preparations should generally be avoided. They are associated with poorer long-term outcomes, dependency risk, and worsening headache patterns.
Preventive Treatment of Migraine
Preventive treatment should be considered when attacks are frequent, disabling, difficult to manage acutely, or when the patient prefers a preventive approach. It is also appropriate when acute medication use is escalating or when migraine subtype and burden justify earlier prevention. The aim is not just to reduce attack count, but to reduce severity, duration, disability, acute medication reliance, and the risk of chronification.
A good preventive trial requires patience. Most oral preventives need titration and should be continued at a therapeutic dose for at least 2–3 months before being judged ineffective. Injectable and biologic treatments may require longer assessment, especially in previous non-responders.
Preventive medication table
| Class | Medication | Starting dose | Target dose | Typical clinical use / key considerations |
|---|---|---|---|---|
| Beta-blocker | Propranolol | 40 mg/day | 120–240 mg/day | Good in hypertension, tremor, anxiety; avoid in asthma or bradycardia |
| Beta-blocker | Metoprolol | 50 mg/day | 100–200 mg/day | Cardioselective alternative |
| Antiepileptic | Topiramate | 15–25 mg/day | 50–200 mg/day | Effective in episodic and chronic migraine; may suit obesity; cognitive adverse effects can limit use |
| Antiepileptic | Valproate / divalproex | 250 mg twice daily | 500–1000 mg/day | Effective but limited by teratogenicity and metabolic effects |
| Tricyclic | Amitriptyline | 10 mg nocte | 25–150 mg nocte | Useful when insomnia, anxiety, or widespread pain sensitivity coexist |
| SNRI | Venlafaxine | 37.5 mg/day | 150 mg/day | Useful in anxiety/depression comorbidity |
| ARB | Candesartan | 4–8 mg/day | 8–16 mg/day | Well tolerated; good in hypertension or older adults |
| Other | Pizotifen | 0.5 mg/day | 1.5 mg/day | Sometimes useful in UK practice; weight gain limits use |
| Other | Memantine | 5 mg/day | 5–20 mg/day | Emerging option; often well tolerated |
| Supplement | Magnesium | 400–600 mg/day | 400–600 mg/day | Useful adjunct, especially in some hormonal patterns |
| Supplement | Riboflavin | 400 mg/day | 400 mg/day | Safe adjunctive option |
| CGRP mAb | Erenumab | 70 mg monthly | 70–140 mg monthly | Receptor-targeting biologic preventive |
| CGRP mAb | Fremanezumab | 225 mg monthly | 225 mg monthly or 675 mg quarterly | Ligand-targeting biologic preventive |
| CGRP mAb | Galcanezumab | 240 mg loading | 120 mg monthly | Ligand-targeting biologic preventive |
| CGRP mAb | Eptinezumab | 100 mg IV quarterly | 100–300 mg IV quarterly | Ligand-targeting biologic with relatively fast onset |
| Gepant | Atogepant | 10–30 mg/day | 30–60 mg/day | Oral preventive for episodic and chronic migraine |
| Gepant | Rimegepant | 75 mg alternate days | 75 mg alternate days | Dual acute + preventive role |
| Botox | OnabotulinumtoxinA | 155 U every 12 weeks | 155–195 U every 12 weeks | Chronic migraine only |
How to choose preventive therapy
Choice should be individualised rather than formulaic. Traditional oral preventives remain useful, especially when they match comorbidities. Beta-blockers suit patients with hypertension or anxiety. Amitriptyline suits patients with insomnia, mood overlay, or pain amplification. Topiramate may be especially attractive in patients where weight loss is not unwelcome, although cognitive adverse effects may limit it. Candesartan is a good pragmatic option in older adults and those with hypertension because of its tolerability. Venlafaxine may help when anxiety or depression is relevant. Valproate is effective but limited by teratogenicity and monitoring issues.
More recent practice increasingly moves CGRP-targeted therapies earlier because of their efficacy and tolerability, although cost and access remain real-world barriers. In chronic migraine, Botox, CGRP monoclonal antibodies, atogepant, and topiramate are all important options, with selection guided by phenotype, comorbidities, prior failures, route preference, and availability.
Preventive selection by patient profile
| Patient profile | Options that often fit best |
|---|---|
| Hypertension | Propranolol, metoprolol, candesartan |
| Anxiety / depression | Amitriptyline, venlafaxine; CGRP therapies if traditional agents poorly tolerated |
| Insomnia | Amitriptyline |
| Obesity | Topiramate; avoid weight-promoting options where possible |
| Chronic migraine | Botox, CGRP monoclonal antibodies, atogepant, topiramate |
| Cardiovascular disease / frail patient | Botox, candesartan, selected beta-blockers, CGRP mAbs depending overall context |
| Multiple prior preventive failures | CGRP mAbs, gepants, Botox, or combination strategies |
What about non-responders?
Failure of one preventive does not mean failure of the whole treatment pathway. One should first confirm that the diagnosis is still correct, that the trial was adequate in dose and duration, and that the pattern is not being confounded by escalating acute medication use or other drivers such as poor sleep, neck pain, or hormonal factors. If one oral preventive fails, switching class is reasonable. If several have failed or tolerance is poor, escalation to Botox or CGRP-targeted therapy becomes increasingly appropriate. In chronic migraine, partial responders may benefit from combination strategies rather than repeated monotherapy changes.
CGRP-Targeted Therapies: A Major Advance
This is one of the most important developments in migraine treatment. CGRP is a key mediator of trigeminovascular signalling, meningeal inflammation, peripheral sensitisation, and attack propagation. Blocking this pathway has transformed both acute and preventive therapy.
Two main CGRP-targeted classes
A. CGRP monoclonal antibodies
These are preventive therapies and are not used for acute treatment.
| Drug | Target | What it blocks | Route / frequency |
|---|---|---|---|
| Erenumab | CGRP receptor | Blocks the receptor itself | Subcutaneous monthly |
| Fremanezumab | CGRP ligand | Binds CGRP before it reaches the receptor | Subcutaneous monthly or quarterly |
| Galcanezumab | CGRP ligand | Binds circulating CGRP ligand | Subcutaneous monthly |
| Eptinezumab | CGRP ligand | Binds CGRP ligand | Intravenous quarterly |
The distinction between receptor and ligand targeting matters conceptually. Erenumab blocks the receptor, preventing CGRP from activating it. Fremanezumab, galcanezumab, and eptinezumab bind the ligand itself, effectively neutralising CGRP before it reaches the receptor. Both approaches reduce CGRP pathway signalling, but at different points in the pathway.
B. Gepants
Gepants are small-molecule CGRP receptor antagonists. Unlike monoclonal antibodies, they can be used for acute treatment, prevention, or both, depending on the drug.
| Drug | Acute treatment | Prevention | Notes |
|---|---|---|---|
| Ubrogepant | Yes | No | Acute only |
| Rimegepant | Yes | Yes | Dual acute + preventive role |
| Atogepant | No | Yes | Oral preventive; episodic and chronic migraine |
| Zavegepant | Yes | No | Nasal acute treatment |
Gepants block the CGRP receptor as small molecules rather than antibodies. They do not cause vasoconstriction, which is one of their biggest practical advantages.
How to choose between mAbs and gepants
Monoclonal antibodies are particularly attractive in patients who prefer monthly or quarterly treatment, have complex polypharmacy, or have renal or hepatic impairment because they have minimal CYP450 interaction issues. Gepants are attractive when an oral option is preferred, when non-vasoconstrictive acute treatment is needed, or when one drug such as rimegepant can serve both acute and preventive roles. Atogepant has become especially important because it provides a migraine-specific oral preventive option for both episodic and chronic migraine.
Which patients are especially suitable?
Patients with cardiovascular disease, triptan contraindications, multiple failed traditional preventives, or substantial migraine disability are often particularly suitable. Patients with significant renal or hepatic impairment or complex polypharmacy may favour monoclonal antibodies because they avoid CYP metabolism. Oral gepants may be preferable when rapid reversibility, oral administration, or flexibility is important.
How long should the trial last?
CGRP-targeted therapies should not be judged too early. A minimum of 3 months is usually required, but 6 months is often a better assessment point for injectables, especially in patients who have failed several previous preventives. This is clinically important because a substantial proportion of patients who appear not to respond at 12 weeks later become responders.
Late responders and non-responders
The concept of late responders matters. Some patients do not show a clear response in the first 3 months but improve later, and some only respond after 24 weeks. Therefore, in a patient tolerating treatment with some sign of trend improvement, it is often reasonable not to abandon therapy too early. Switching from one CGRP monoclonal antibody to another may still be worthwhile, and combining an acute gepant with a preventive mAb can also be rational in selected patients.
Comparative points: gepants vs CGRP monoclonal antibodies
| Feature | Oral gepants | CGRP monoclonal antibodies |
|---|---|---|
| Route | Oral | Subcutaneous or IV |
| Onset | Often within 1 week | Typically 1–4 weeks |
| Half-life | Shorter | Long |
| Reversibility | Rapid | Slow |
| Dual acute/preventive role | Yes, with rimegepant | No, prevention only |
| Drug interactions | CYP3A4 issues matter | Minimal |
| Suitability in polypharmacy | Good, but interaction check needed | Excellent |
Non-Pharmacological Treatments
Non-pharmacological management is an important part of comprehensive migraine care, not an optional extra. It is especially valuable in patients who prefer to reduce medication burden, have contraindications, are pregnant, or need a broader multimodal plan. The strongest evidence supports behavioural therapies, acupuncture, regular exercise, and sensible trigger management.
Behavioural and psychological strategies such as cognitive behavioural therapy, biofeedback, relaxation training, and mindfulness-based approaches can reduce attack frequency, improve disability, and help patients regain control over a highly disruptive condition. Trigger management should be practical rather than rigid: alcohol, caffeine fluctuation, dehydration, missed meals, sleep disturbance, hormonal change, bright light, strong odours, and stress are common triggers, but patients should avoid becoming excessively restrictive. Acupuncture has one of the stronger evidence bases among non-pharmacological preventive options and is especially relevant where patients prefer non-drug prevention. Regular aerobic exercise, dietary regularity, selected supplementation, and physiotherapy may also contribute meaningfully in the right patient.
FDA-Cleared and Related Neuromodulation Devices
Neuromodulation has become increasingly important because it offers non-systemic therapy without the vasoconstrictive limitations of triptans or the organ and interaction issues of some medications. These devices are especially relevant in pregnancy, cardiovascular disease, medication intolerance, and patients seeking non-drug approaches.
Device comparison table
| Device | Role | Target | Best use |
|---|---|---|---|
| Cefaly (e-TNS) | Acute and preventive | Trigeminal nerve V1 | Daily prevention and acute treatment; very well tolerated |
| Nerivio (REN) | Acute and preventive | Upper arm peripheral nerves / conditioned pain modulation | Useful for patients preferring arm-based device |
| sTMS | Acute and preventive | Occipital cortex | Particularly useful in migraine with aura |
| gammaCore (nVNS) | Preventive and selected acute use | Cervical vagus nerve | Prevention; useful where drug interactions or medication intolerance matter |
| TENS | Adjunctive acute and preventive use | Peripheral or cervical targets | Lower-cost adjunct |

Cefaly delivers external trigeminal nerve stimulation via a forehead electrode and is one of the most practical devices for both acute and preventive use. Nerivio is a smartphone-controlled armband using remote electrical neuromodulation and is particularly appealing to patients who dislike head-based devices. Single-pulse transcranial magnetic stimulation is especially relevant in migraine with aura because it targets cortical excitability and cortical spreading depression. gammaCore stimulates the cervical vagus nerve and offers a non-drug option in selected patients, although contraindications must be respected. TENS is not migraine-specific in regulatory terms but remains clinically relevant as a lower-cost neuromodulation strategy.
OnabotulinumtoxinA (Botox) for Chronic Migraine
Botox is one of the main procedural pillars in chronic migraine management and one of the key strengths of a specialist interventional migraine service. It is FDA-approved specifically for chronic migraine, not episodic migraine, and acts through sensory mechanisms rather than simply muscle relaxation. By cleaving SNAP-25 and interfering with neurotransmitter release, it reduces the release of CGRP, glutamate, and substance P from sensory nerve endings and helps reduce peripheral and central sensitisation.
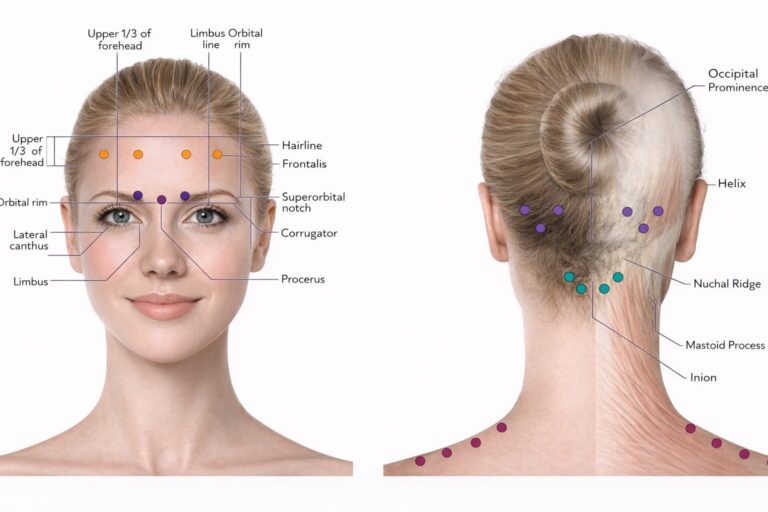
The PREEMPT protocol remains the evidence-based standard. This involves 31 fixed injection sites delivering 155 units, with the option to extend up to 195 units using a follow-the-pain approach. Treatment is given every 12 weeks. Response should not be judged too early: patients often require up to three cycles before treatment failure should be considered.
At Pain Spa, Botox for chronic migraine is an important part of the treatment pathway. Proper patient selection, accurate technique, adherence to PREEMPT principles, and the ability to tailor treatment where appropriate all matter. Patients with chronic migraine, coexistent cervical or trapezial pain, scalp allodynia, or mixed head and neck symptom patterns may particularly benefit from specialist assessment.
Greater Occipital Nerve Blocks
Greater occipital nerve block is one of the most useful interventional procedures in migraine practice. The greater occipital nerve arises primarily from C2 and interacts functionally with trigeminal pathways through the trigeminocervical complex. This explains why blocking an occipital nerve can influence frontal migraine pain. Clinically, GON block has roles in acute migraine, bridging therapy, preventive support, status migrainosus, and difficult treatment transitions.
Evidence for acute migraine treatment is strong enough that GON block has received a Level A recommendation for acute migraine in emergency care guidance. Evidence for prevention is also supportive, especially in chronic migraine. Bilateral blocks are commonly used in migraine because the aim is modulation of the trigeminocervical system rather than simply numbing one local pain point. Local anaesthetic alone is generally sufficient; corticosteroids are not routinely recommended for migraine blocks because they add risk without clear added benefit in this setting.
At Pain Spa, greater occipital nerve blocks are an important part of the migraine pathway, particularly when a patient is waiting for Botox to take effect, when acute escalation needs to be interrupted, when occipital tenderness is prominent, or when a patient is not suitable for systemic escalation. Real-time ultrasound guidance improves precision and is especially valuable in difficult anatomy and in advanced interventional practice.
Pulsed Radiofrequency of the Greater Occipital Nerve
Pulsed radiofrequency occupies an important niche between repeated nerve blocks and destructive thermal lesioning. Unlike conventional thermal radiofrequency, PRF is designed to modulate neural function without creating a destructive lesion, usually operating at temperatures of 42°C or below. This makes it particularly attractive in migraine, where the goal is durable neuromodulation rather than denervation.
The best candidates are patients with chronic migraine, clear occipital tenderness, a positive response to diagnostic GON block, inadequate response to conventional preventive treatment, or only short-lived benefit from repeated nerve blocks. Available evidence supports PRF as a useful step-up treatment in selected refractory patients, with sustained relief often lasting several months.
PRF in migraine: practical summary
| Key point | PRF in migraine |
|---|---|
| Role | Refractory chronic migraine |
| Best suited to | Patients with occipital tenderness and positive response to GON block |
| Advantage | More sustained relief than repeated short-acting blocks in selected patients |
| Limitation | Not a first-line treatment; requires careful selection |
At Pain Spa, Dr Krishna is an expert at performing PRF treatment and we offer this as an advanced option within the migraine pathway for selected refractory patients, especially when occipital nerve blocks help but wear off too quickly.
Supraorbital and Auriculotemporal Nerve Blocks
Supraorbital nerve block is particularly relevant in frontal-predominant migraine, where pain is concentrated over the forehead and anterior scalp. The supraorbital nerve is a terminal branch of V1, so blocking it targets trigeminal afferent traffic more directly in that region. SON blocks have evidence for acute benefit and may be even more useful when combined with GON blocks, especially when frontal and occipital symptoms coexist.
Auriculotemporal nerve block is more relevant in temporal-predominant migraine. The auriculotemporal nerve, a branch of V3, supplies the temporal scalp and adjacent tissues. Isolated evidence is more limited than for GON block, but ATN block is well recognised within multiple cranial nerve block protocols and is especially useful where the pain distribution repeatedly localises to the temple region.
A major strength of specialist migraine intervention is the ability to move beyond standard occipital blocks and Botox alone. In patients with frontal, temporal, multifocal, or atypical pain distribution, combined cranial nerve block strategies may offer more anatomically matched treatment than a one-size-fits-all approach. For patients who fail GON blocks alone, a multiple cranial nerve block protocol targeting the GON, lesser occipital nerve, SON, supratrochlear nerve, and ATN can be the next interventional step.
Sphenopalatine Ganglion Blocks
SPG block is another important interventional option, particularly in acute migraine, status migrainosus, or attacks with strong frontal or autonomic features. The sphenopalatine ganglion is a parasympathetic ganglion within the pterygopalatine fossa, functionally linked to trigeminal pain pathways and to autonomic features such as lacrimation and nasal symptoms. That is why it is a rational target in selected migraine patients.
Evidence is more mixed than for GON block, but the procedure is widely used in clinical practice and appears particularly valuable in status migrainosus and transitional treatment settings. Repetitive SPG blockade has also shown preventive benefit in some studies, although evidence certainty remains lower than for Botox or GON block. Multiple techniques are available, including transnasal catheter techniques, traditional applicator approaches, and suprazygomatic approaches.
Integration of Interventional Approaches and the Pain Spa Pathway
One of the strengths of a specialist migraine service is that these procedures are not used as isolated tricks, but as part of a structured interventional pathway.
| Clinical scenario | Recommended interventional approach |
|---|---|
| First-line interventional treatment for chronic migraine prevention | Botox using PREEMPT protocol every 12 weeks |
| Acute breakthrough headache on prevention | Bilateral GON block; consider adding SON block for frontal pain |
| Status migrainosus | GON block with or without medical therapy; SPG block if frontal/autonomic features are prominent |
| Waiting for Botox effect | GON blocks monthly or as needed for 2–3 months |
| Refractory to Botox and CGRP-targeted prevention | GON PRF if diagnostic block has been positive |
| Short-lived response to repeated GON blocks | GON PRF |
| Occipital-predominant migraine | GON blocks; escalate to PRF if more sustained relief is needed |
| Frontal-predominant migraine | Add SON blocks or consider SPG block |
| Temporal-predominant migraine | Add auriculotemporal nerve block |
| Diffuse or multifocal cranial pain | Multiple cranial nerve block protocol |
Migraine treatments offered at Pain Spa
| Treatment | Offered at Pain Spa |
|---|---|
| Botox for chronic migraine | ✅ |
| Greater occipital nerve blocks | ✅ |
| Pulsed radiofrequency of the greater occipital nerve | ✅ |
| Supraorbital nerve block | ✅ |
| Auriculotemporal nerve block | ✅ |
| Sphenopalatine ganglion block | ✅ |
| Combined cranial nerve block protocols | ✅ |
These treatments should be presented clearly as part of a specialist ultrasound-guided interventional migraine service, with emphasis on careful patient selection, precise real-time guidance where appropriate, and an integrated treatment pathway rather than disconnected procedures.
Special Situations
Migraine in pregnancy
This article is not intended to reproduce the full pregnancy discussion in detail because a dedicated separate article is planned. However, migraine in pregnancy requires a more cautious framework. Non-pharmacological measures become even more important, and non-systemic options such as neuromodulation devices and peripheral nerve blocks may be particularly valuable. Drug choices are more limited, and the balance between maternal benefit and fetal safety must be considered carefully. A dedicated article on migraine management in pregnancy should be linked from the final website version.
Medication overuse headache
Medication overuse headache is a common reason migraine becomes more frequent, more refractory, and more confusing clinically. It should be recognised as an important complicating factor rather than a side note. Management usually involves patient education, rational withdrawal of the overused acute medication, and optimisation of preventive therapy. Interventional strategies such as GON blocks may help as bridging tools during this process. A separate detailed article on medication overuse headache should also be linked from the final website version.
Conclusion
Migraine management has changed profoundly in recent years. Accurate diagnosis remains fundamental, but the therapeutic landscape is now far broader and more sophisticated than it once was. Evidence-based acute treatment includes NSAIDs, triptans, gepants, ditans, and antiemetics used in a stratified way. Prevention now spans traditional oral agents, supplements, Botox, CGRP monoclonal antibodies, and oral gepants. Behavioural therapies, acupuncture, lifestyle regularity, and neuromodulation devices provide important non-drug options. Interventional approaches — particularly Botox, greater occipital nerve blocks, pulsed radiofrequency, supraorbital and auriculotemporal blocks, and SPG block — allow treatment to be tailored more precisely to headache phenotype, prior treatment response, and clinical need.
At Pain Spa, migraine should be approached not as a single prescription problem, but as a condition requiring correct diagnosis, evidence-based drug selection, careful review of non-response, and access to a full range of advanced interventional options delivered with specialist expertise. That is the framework most likely to give patients meaningful and sustained improvement.