Knee Arthritis Pain: New Treatments on the Horizon and Advanced Options Currently Available

New Treatments for Knee Arthritis: What’s Coming – and What Can Help Now
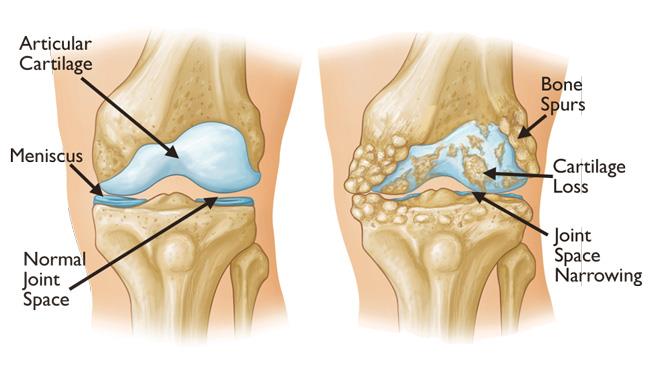
Knee osteoarthritis is one of the most common causes of chronic pain and reduced mobility. Many patients struggle with persistent pain on walking, stairs or standing, and some gain limited relief from painkillers, physiotherapy or lifestyle changes alone.
A recent national media report highlighted several new developments on the horizon. Some of these therapies may eventually change arthritis care, but it is important to separate what is still experimental from what is already available now in specialist clinics.
Experimental & emerging treatments (not yet routine care)
The treatments below are promising, but most are still in research phases. They may be available only within clinical trials, and their long-term safety and effectiveness still need to be confirmed.
1) Neurotrophin inhibitors (LEVI-04): targeting pain at its source
The report described a new class of drugs known as neurotrophin inhibitors, focusing on an investigational injection called LEVI-04 for symptomatic knee osteoarthritis.
In osteoarthritis, a nerve-growth protein called neurotrophin-3 (NT-3) may become overactive in damaged joints. Higher NT-3 levels can encourage pain-sensing nerves within the knee to grow and become hypersensitive, meaning everyday movements such as walking, standing or stair climbing can trigger severe pain.
LEVI-04 is designed to block NT-3, reducing amplification of pain signals coming directly from the knee. Because it is injected into the joint, it is intended to work locally and potentially reduce whole-body side effects seen with long-term pain medication.
Early trial results reported substantial improvements in pain and function. Researchers are also exploring whether it might influence joint structure and cartilage deterioration, although this remains under investigation.
Current status: Experimental – Phase 3 trial results awaited; not yet approved or routinely available outside research settings.
2) GLP-1 “slimming jabs”: possible benefits beyond weight loss
The report also discussed GLP-1 weight-loss injections as a potential approach for knee osteoarthritis. Excess weight increases the mechanical load across the knee and can accelerate cartilage wear, worsening pain and stiffness.
In addition to weight reduction, experts suspect GLP-1 drugs may offer added benefits through anti-inflammatory effects, although the mechanism is not yet fully understood. Research cited in the report suggested patients receiving these injections were less likely to progress to joint replacement surgery.
Researchers are also exploring whether injecting GLP-1–based treatments directly into the joint could enhance benefits, but this is not currently routine practice.
Current status: Experimental for osteoarthritis – not included in arthritis prescribing guidelines; intra-articular use remains investigational.
3) “Smart” artificial cartilage gel: responsive drug delivery
Researchers have developed a soft, gel-like material designed to mimic natural cartilage while also releasing medication precisely when needed. The idea is that it can detect chemical changes during an arthritis flare-up and release anti-inflammatory drugs in response.
This approach could potentially provide more continuous symptom control while reducing side effects associated with medicines taken by mouth.
Current status: Early-stage development – laboratory and pre-clinical research; not available for routine clinical use.
4) Immunotherapy-style vaccine targeting IL-6 inflammation
Another development described in the report is an experimental vaccine targeting interleukin-6 (IL-6), an inflammatory protein linked to cartilage breakdown and joint inflammation in osteoarthritis.
In a small early study, patients receiving the vaccine had lower IL-6 levels than those given placebo. However, experts urge caution because similar treatments have not consistently delivered strong results in previous arthritis trials, and benefits may apply only to a subset of patients.
Current status: Experimental – early human research only; not ready for routine clinical practice.
5) Brazilian herbal therapy (Joseph’s Coat): animal research only
The report also mentioned an early study of a Brazilian medicinal plant (Alternanthera littoralis, sometimes known as Joseph’s Coat). In animal models, compounds from the plant appeared to reduce inflammation, swelling, pain and stiffness.
Although intriguing, animal research cannot be assumed to translate directly into effective human treatment, and clinical trials would be needed to establish safety, dosing and benefit.
Current status: Experimental – animal research stage only; not studied clinically in humans.
Available now: advanced injection-based and interventional treatments
While emerging therapies are exciting, many patients do not need to wait for future treatments to get meaningful relief. Modern interventional pain medicine can target both the joint environment and the pain pathways around the knee, helping to reduce pain, improve mobility, and delay or avoid surgery in selected cases.
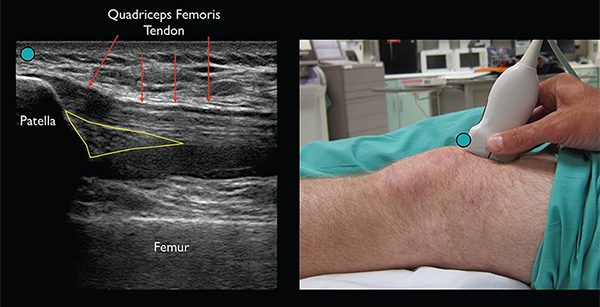
At Pain Spa, treatments are delivered with a focus on precision and safety using real-time imaging guidance where appropriate, particularly ultrasound.
Specialist knee pain treatments available at Pain Spa
Pain Spa offers a comprehensive range of advanced, evidence-based treatments for knee osteoarthritis and chronic knee pain, tailored to the individual patient following specialist assessment.
- Ultrasound-guided steroid injections for inflammatory flare-ups
- Viscosupplementation (hyaluronic acid injections)
- N-Stride PRP (platelet-rich plasma) injections
- Arthrosamid® polyacrylamide hydrogel injections
- Genicular nerve blocks
- Cooled radiofrequency (RF) treatment of the genicular nerves
Dr Krishna has extensive experience in performing these procedures under real-time ultrasound guidance, allowing precise needle placement, improved safety, and more consistent clinical outcomes compared with landmark-based techniques.
Dr Krishna was the first clinician in the UK to perform cooled radiofrequency treatment for knee pain, and continues to use this technique as part of a personalised approach aimed at reducing pain, improving function, and delaying or avoiding surgery where possible.
Arthrosamid® hydrogel injection
Arthrosamid is a long-acting hydrogel injection placed into the knee joint under ultrasound guidance. It is designed to provide durable cushioning and improved joint mechanics, reducing friction and stress that contribute to pain.
Current status: Available now in specialist pain clinics.

N-Stride PRP (platelet-rich plasma)
PRP uses a small blood sample processed to concentrate platelets, which contain growth factors and signalling molecules. The PRP is then injected into the knee to help modulate inflammation and support tissue healing, particularly in early to moderate osteoarthritis.
Current status: Available now in specialist pain clinics.
Genicular nerve blocks and cooled radiofrequency (RF)
For some patients, knee pain is driven by overactive sensory nerves around the joint, even when the joint itself has been treated. Genicular nerve blocks place local anaesthetic around these nerves under imaging guidance and can provide short-term relief while confirming whether the nerves are a major contributor to pain.
Patients who respond well may benefit from cooled radiofrequency (RF), which reduces pain transmission along the genicular nerves without damaging the knee joint. Cooled RF creates a larger, more consistent treatment effect than standard RF, and pain relief commonly lasts around 6–12 months or longer.
Current status: Available now in specialist pain clinics.

Steroid injections and viscosupplementation
Ultrasound-guided steroid injections can be helpful during inflammatory flare-ups, particularly when swelling is prominent, but are usually used selectively rather than repeatedly. Viscosupplementation (hyaluronic acid) aims to improve lubrication and shock absorption and may reduce pain and improve mobility for some patients.
Current status: Available now in selected cases.
Summary: treatments, typical benefit and current status
| Treatment | What it targets / how it works | Typical benefit | Typical duration | Current status |
|---|---|---|---|---|
| Neurotrophin inhibitors (e.g. LEVI-04) | Blocks NT-3 nerve-growth signalling to reduce pain amplification within the knee | Marked reduction in pain and stiffness in early trials | Still being studied | Experimental – Phase 3 trials ongoing |
| GLP-1 weight-loss injections | Reduces joint load via weight loss; possible anti-inflammatory effects | Reduced progression to joint replacement in observational studies | Ongoing while treatment continues | Experimental for arthritis |
| Smart artificial cartilage gel | Artificial cartilage with inflammation-responsive drug release | Potential targeted pain and inflammation control | Unknown | Pre-clinical – laboratory research only |
| IL-6 immunotherapy vaccine | Targets inflammatory pathways involved in cartilage damage | Reduced inflammatory markers in small studies | Unknown | Experimental – early human trials |
| Brazilian herbal therapy (Joseph’s Coat) | Plant-based anti-inflammatory compounds (animal studies) | Reduced pain and inflammation in animal models | Unknown | Experimental – animal research only |
| Arthrosamid® hydrogel injection | Provides long-lasting cushioning and joint stabilisation | Sustained pain relief and improved function | Typically 2–3+ years | Available now – ultrasound-guided by Dr Krishna at Pain Spa |
| N-Stride PRP | Autologous growth factors to modulate inflammation and healing | Pain reduction and functional improvement | Approximately 6–12 months | Available now – ultrasound-guided by Dr Krishna |
| Genicular nerve blocks | Temporarily blocks pain-carrying sensory nerves | Short-term relief and diagnostic clarity | Days to weeks | Available now – imaging-guided by Dr Krishna |
| Cooled radiofrequency (genicular RF) | Reduces pain transmission by treating genicular nerves | Significant pain reduction and improved mobility | Typically 6–12+ months | Available now – ultrasound/fluoroscopy-guided by Dr Krishna |
| Steroid injections (ultrasound-guided) | Reduces active joint inflammation during flares | Short-term pain relief | Weeks to a few months | Available now – selective use at Pain Spa |
| Viscosupplementation (hyaluronic acid) | Improves lubrication and shock absorption | Variable pain relief and improved movement | Several months (variable) | Available now – imaging-guided where appropriate |
Key takeaway
Several exciting therapies are in development, including targeted pain-pathway injections, metabolic approaches and novel drug-delivery materials. However, most remain experimental and are not yet accessible in routine care.
The encouraging news is that there are already multiple effective, minimally invasive options available now. A specialist assessment can help determine which treatment (or combination of treatments) is most appropriate to reduce pain, improve mobility and support independence.
If you would like to explore any of the above treatments, please contact Pain Spa at clinic@painspa.co.uk or via our website www.painspa.co.uk.
Medical information on this page is for general education and does not replace personalised medical advice. Suitability of any treatment depends on clinical assessment, imaging findings, and individual factors.