TMJ Pain and Bruxism: Why Muscle Dysfunction Is Often the Hidden Driver

TMJ Dysfunction and Myofascial Pain: Why the Muscles — Not the Joint — Are Often the Real Pain Generator
Temporomandibular joint (TMJ) dysfunction is a common cause of facial pain, jaw discomfort, headaches and ear-related symptoms. Many people are told they have “TMJ pain” and naturally assume the joint itself must be the problem, but in clinical practice the dominant pain generator is frequently muscular rather than intra-articular.
Understanding whether symptoms are driven by the joint (arthrogenic), the surrounding muscles (myofascial), or a combination of both is critical, because treatment strategies differ significantly. At Pain Spa, assessment is mechanism-based: the aim is to identify the dominant source of pain before recommending targeted intervention.
TMJ Anatomy — Beyond the Joint
The joint
The temporomandibular joint is a synovial ginglymoarthrodial joint, meaning it performs both hinge (rotational) and sliding (translational) movements. This dual function allows smooth opening, closing and lateral jaw movement.
Key components include the mandibular condyle, glenoid fossa, articular eminence, fibrocartilaginous disc, capsule and synovium, and the retrodiscal (bilaminar) zone. Disc displacement is relatively common and may be seen in asymptomatic individuals, so structural findings on imaging do not always correlate with pain; clinical assessment remains central to diagnosis.

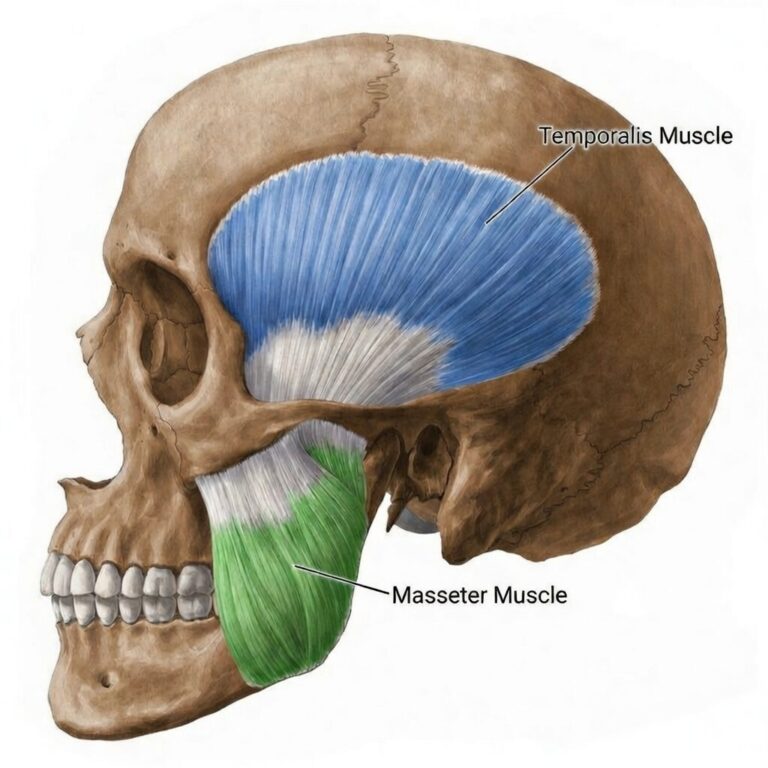
The Muscles of Mastication — Often the True Pain Source
In many patients, the muscles surrounding the joint are the principal source of pain rather than the joint itself.
Sustained overactivity of these muscles may lead to local hypoxia, trigger point formation, peripheral sensitisation and, in some patients, secondary central amplification of pain.
Myofascial TMJ Pain — The Overlooked Driver
Temporomandibular disorders are broadly divided into myofascial (muscle-driven) and arthrogenic (joint-driven) presentations. In myofascial pain, muscle overuse can lead to local hypoxia, accumulation of inflammatory mediators and a pain–spasm–pain cycle, with peripheral sensitisation and, in chronic cases, central sensitisation.
Common contributing factors include bruxism, psychological stress, postural strain, dental procedures and jaw overuse.
Teeth Grinding (Bruxism) and Its Role in TMJ Pain and Headaches
Bruxism — repetitive clenching or grinding of the teeth — is one of the most significant contributors to myofascial temporomandibular pain. It may occur during sleep or while awake, often subconsciously in response to stress. Unlike normal chewing, bruxism involves sustained muscle contraction, placing prolonged load on the muscles of mastication.
How bruxism leads to pain
Bruxism and headache patterns
If bruxism is the dominant driver, treating the joint alone will not resolve symptoms.
Diagnosis
Accurate diagnosis is central to effective management. Important features in the history include bruxism or clenching, morning jaw tightness, headaches on waking, psychological stress, trauma, recent dental procedures, and locking or catching sensations.
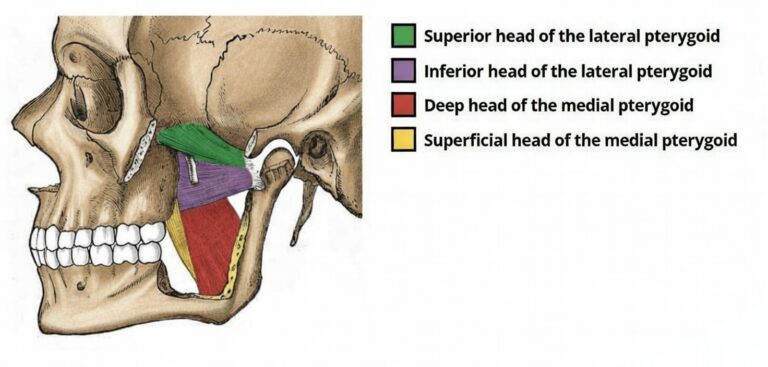
A structured examination includes facial symmetry, mouth opening measurement, deviation on opening, palpation of masseter, temporalis and pterygoids, joint line palpation, and loading tests. Reproduction of the patient’s familiar pain during muscle palpation strongly supports a myofascial origin.
MRI can be useful for disc displacement, joint effusion and inflammatory arthritis; however, imaging abnormalities are common in asymptomatic individuals and normal scans do not exclude muscle-driven pain.
In selected cases, targeted diagnostic injections can help clarify the dominant pain source, for example local anaesthetic injection into masseter or temporalis, lateral pterygoid injection, auriculotemporal nerve block, or intra-articular TMJ injection. Significant relief after muscle injection supports a myofascial origin.
Treatment Overview
TMJ-related pain is best treated using a mechanism-based approach. The right treatment depends on whether symptoms are primarily driven by muscle overactivity, joint inflammation, neuropathic features, or a combination.
Conservative Management
First-line measures commonly include education, behavioural modification, occlusal splints (when appropriate), physiotherapy, postural correction and stress management.
Trigger Point Injections
Trigger point injections using local anaesthetic, with or without a small dose of corticosteroid, may help break the pain–spasm cycle, reduce local inflammation and provide diagnostic clarity. Common muscles treated include masseter, temporalis, medial pterygoid and, in selected cases, lateral pterygoid.
Intra-Articular TMJ Injections
Intra-articular injections are considered when there is confirmed arthrogenic pain or inflammatory synovitis. Options may include local anaesthetic and corticosteroid; joint injections are unlikely to help when muscle overactivity is the primary driver.
Botulinum Toxin Injections
Botulinum toxin can be an effective treatment in selected cases of chronic myofascial TMJ pain, particularly where excessive muscle activity and bruxism are major contributors.
It works by temporarily reducing acetylcholine release at the neuromuscular junction, leading to controlled reduction in muscle contraction. In addition, it appears to reduce the release of inflammatory neuropeptides involved in pain signalling, contributing to its analgesic effect beyond simple muscle relaxation.
Indications
Botulinum toxin may be considered when:
- Severe bruxism is contributing to muscle pain
- Chronic myofascial TMD persists despite conservative treatment
- Recurrent muscle spasm continues after trigger point therapy
It is not first-line treatment and is not indicated for painless joint clicking.
Target Muscles
Commonly treated muscles include:
- Masseter
- Temporalis
- Lateral pterygoid in selected cases
Injection of the lateral pterygoid requires particular anatomical expertise due to its depth and proximity to important structures.
Expected Effects
Patients typically notice reduced clenching intensity, decreased muscle tension and gradual reduction in pain over 2–4 weeks. The goal is reduction of hyperactivity rather than complete muscle paralysis.
Duration and Risks
The effect usually lasts around 3–4 months. Some patients experience longer benefit with repeated treatments. Possible side effects include temporary chewing fatigue, mild asymmetry, or transient weakness. When administered carefully and in appropriate doses, botulinum toxin is generally well tolerated.
Nerve Blocks
In selected patients, targeted nerve blocks can play both a diagnostic and therapeutic role in the management of TMJ-related pain.
The nerves most commonly targeted include:
Auriculotemporal nerve
Masseteric nerve
Deep temporal nerves
Mandibular division (V3) in refractory or complex cases
These interventions are particularly helpful when the distribution of pain suggests a dominant neural pathway or when it is unclear whether symptoms are primarily muscular, articular, or neuropathic.
A carefully performed nerve block can temporarily interrupt peripheral pain signalling, help confirm the principal pain generator, and in some cases provide meaningful short- to medium-term relief.
Nerve blocks are not first-line treatment but can be valuable in appropriately selected patients, especially when conservative measures and local muscle therapies have not provided sufficient improvement.
When Is Surgery Appropriate?
Surgery is reserved for true disc locking, structural joint damage, severe degenerative arthropathy or trauma. Surgery does not treat muscle-driven pain and is not appropriate for primary myofascial TMD.
The Pain Spa Approach
At Pain Spa, TMJ dysfunction is assessed through a structured, mechanism-based framework to determine whether the dominant pain generator is muscular, articular, or mixed. Dr Krishna has extensive experience in ultrasound-guided muscle injections, advanced lateral pterygoid techniques, botulinum toxin therapy and targeted nerve blocks. Treatment is individualised and designed to reduce pain while avoiding unnecessary procedures.
Frequently Asked Questions (FAQ)
Is TMJ pain always caused by the joint? No. In many patients, the muscles of mastication are the dominant pain generator, with the joint playing a secondary role or being structurally normal.
Does clicking mean the joint is damaged? Not necessarily. Clicking is common and may occur even in people without pain. The key issue is whether clicking is associated with pain, locking or functional limitation.
Can I have severe pain with a normal MRI? Yes. Myofascial TMJ pain often has normal imaging because the problem is muscle and nerve sensitisation rather than structural joint damage.
Will a joint injection help if my pain is muscular? Joint injections are most helpful when there is true intra-articular inflammation or arthrogenic pain. If muscle is the primary driver, muscle-focused treatments (physiotherapy, trigger point injections, Botox, etc.) are more likely to help.
Is botulinum toxin safe and how long does it last? When used appropriately by experienced clinicians, botulinum toxin is generally well tolerated. Effects typically last around 3–4 months, with gradual improvement over 2–4 weeks.
Will I need surgery? Most patients with primarily myofascial TMJ pain do not require surgery. Surgical treatments are generally reserved for true mechanical joint problems such as locking or significant structural pathology.
Next Step
If you are experiencing jaw pain, facial pain, headaches linked to clenching, or persistent symptoms despite dental and medical investigations, a mechanism-based TMJ assessment may help identify the dominant pain generator and guide targeted treatment options. To book a consultation, please contact Pain Spa at clinic@painspa.co.uk or visit www.painspa.co.uk for further information.
Medical disclaimer: This article is for education only and does not replace personalised medical advice. If you have acute or rapidly worsening symptoms, significant swelling, fever, neurological symptoms, unexplained weight loss, or other red-flag features, seek urgent medical review.