Vaginismus: Causes, Pelvic Floor Hypertonicity and the Role of Botox Treatment

Vaginismus: Understanding the Condition, Pelvic Floor Hypertonicity, Pudendal Nerve Involvement and the Role of Botox Treatment
At Pain Spa, we approach vaginismus through a structured, multidisciplinary, evidence-based framework.
Introduction
Vaginismus is one of the most distressing and misunderstood causes of painful or impossible vaginal penetration. It affects intimate relationships, self-esteem, fertility planning, and mental wellbeing. Many women suffer silently for years before seeking help.
Patients frequently report:
- Inability to tolerate intercourse
- Severe pain or “hitting a wall” sensation with penetration
- Inability to insert tampons
- Fear of gynaecological examinations
- Panic or involuntary tightening during attempted penetration
Importantly, vaginismus is not a voluntary condition, and it is not simply psychological. It is a complex interaction between:
- Pelvic floor muscle hypertonicity
- Pain sensitisation
- Fear-avoidance cycles
- Nervous system dysregulation
- Sometimes pudendal nerve involvement
What Is Vaginismus?
Vaginismus is defined as:
Persistent or recurrent difficulty allowing vaginal entry of a penis, finger, tampon, or medical instrument due to involuntary pelvic floor muscle contraction, despite the woman’s desire to permit penetration.
Historically described as spasm of the outer third of the vagina, more recent classifications place it under Genito-Pelvic Pain/Penetration Disorder (DSM-5), although this merging with dyspareunia has created diagnostic confusion.
Clinical Characteristics
- Involuntary contraction of levator ani and bulbospongiosus
- Guarding at the introitus
- Anxiety or panic response
- Sometimes burning pain
- Often complete inability to permit examination
Primary vs Secondary
- Primary vaginismus: Penetration has never been possible
- Secondary vaginismus: Develops after pain, trauma, infection, childbirth, surgery, menopause, or relationship stress
In more severe cases, the condition may lead to prolonged inability to achieve penetrative intercourse, sometimes extending over several years.
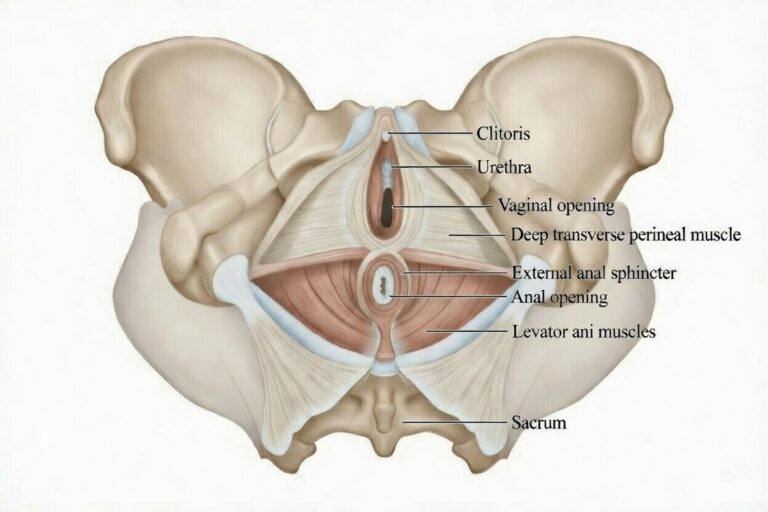
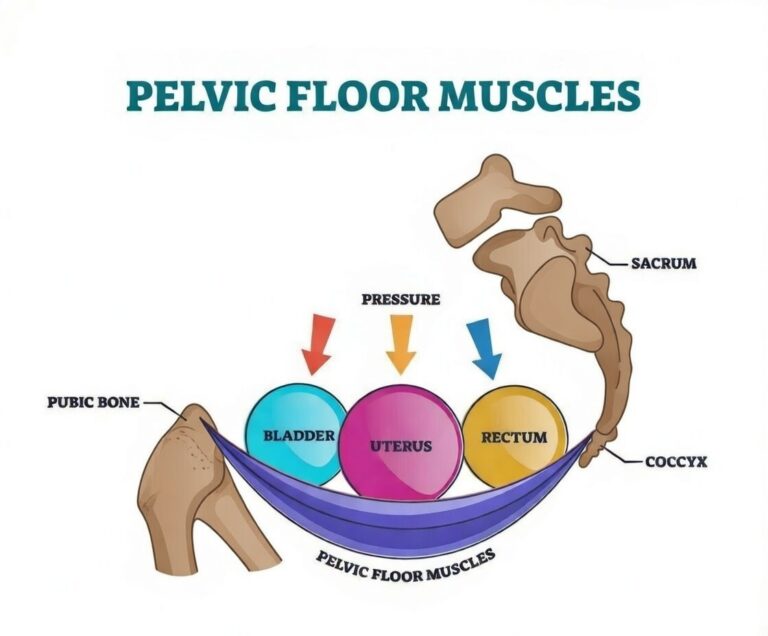
The Pelvic Floor: Anatomy and Biomechanics
Understanding vaginismus requires understanding pelvic floor anatomy.
Core Muscular Components
The pelvic floor consists of layered muscles:
Deep Layer – Levator Ani Complex
- Pubococcygeus
- Puborectalis
- Iliococcygeus
These muscles form the muscular diaphragm of the pelvis.
Superficial Layer
- Bulbospongiosus
- Ischiocavernosus
- Superficial transverse perineal
These surround the vaginal opening and perineal body.
Obturator Internus
Though not part of the pelvic floor proper, it contributes to pelvic sidewall tension and trigger points.
What Happens in Vaginismus?
In vaginismus:
- Resting tone is elevated
- Reflex contraction occurs with anticipated penetration
- Trigger points may develop
- The introitus narrows
- Guarding becomes habitual
Over time, this hypertonicity becomes neurophysiologically reinforced, meaning the nervous system expects penetration to be threatening.
Pelvic Floor Hypertonicity: The Core Mechanism
Pelvic floor hypertonicity is central to vaginismus.
The condition is best understood through the fear-avoidance model of pain:
- Painful attempt or anticipated pain
- Catastrophic expectation
- Defensive muscle contraction
- Failed penetration
- Reinforced fear
This becomes a vicious cycle.
With repeated guarding:
- Muscles shorten
- Myofascial trigger points develop
- Local ischemia occurs
- Peripheral sensitisation increases
Eventually, even light touch can trigger spasm.
This explains why many women say: “I want to relax, but my body won’t let me.”
The Role of the Pudendal Nerve
The pudendal nerve (S2–S4) provides:
- Motor supply to pelvic floor muscles
- Sensory supply to vulva and perineum
In complex cases, there may be:
- Pudendal nerve sensitisation
- Compression from hypertonic pelvic muscles
- Neurogenic inflammation
Botulinum toxin has two important potential mechanisms:
- Muscle relaxation → reduces mechanical compression
- Reduction of neuropeptides (including substance P) → may reduce peripheral sensitisation
In patients with burning pain, sitting intolerance, or radiation to the perineum, pudendal involvement should be assessed carefully.
Vaginismus vs Vulvodynia vs Vestibulodynia
Dyspareunia
- Symptom of painful intercourse
- Can arise from multiple causes
Proper differentiation is essential before considering Botox.
Conventional Treatments for Vaginismus
Management of vaginismus is almost always multimodal, and in many cases conservative treatment is highly successful. However, the success of these approaches depends on severity, duration of symptoms, degree of muscle hypertonicity, and psychological overlay.
1. Pelvic Floor Physiotherapy
Specialist pelvic health physiotherapy is often the first-line intervention. Unlike general physiotherapy, pelvic physiotherapists are trained in:
- Internal assessment of pelvic floor muscle tone
- Identification of trigger points
- Graded desensitisation techniques
- Breathing–pelvic floor coordination
- Biofeedback-guided relaxation
In mild to moderate vaginismus, physiotherapy alone may gradually reduce resting tone and allow penetration over time.
However, in severe cases, the muscle contraction may be so strong that internal examination itself is impossible — limiting progress.
2. Graduated Vaginal Dilator Therapy
Dilator therapy works on the principle of graded exposure and neuromuscular retraining.
The patient progresses gradually through increasing dilator sizes, allowing:
- Desensitisation of the introitus
- Reduction in fear response
- Muscle relaxation retraining
- Increased confidence
This approach is conceptually similar to exposure therapy used in anxiety disorders.
However, in patients with severe spasm, dilators may not be tolerable at all without prior muscle relaxation.
3. Psychological Therapy
Psychological therapy plays a key role because vaginismus often involves:
- Fear-avoidance cycles
- Catastrophic anticipation of pain
- Sexual trauma history
- Shame and stigma
- Relationship anxiety
The fear-avoidance model described in clinical literature shows how anticipation of pain leads to defensive muscle contraction, reinforcing failure of penetration attempts.
In early-stage vaginismus, cognitive behavioural therapy (CBT), sex therapy, and psychoeducation may be sufficient.
However, when the pelvic floor is already chronically hypertonic, psychological therapy alone cannot reverse muscle spasm.
4. Topical Treatments
Topical lignocaine has been reported as an adjunct to reduce superficial hyperesthesia.
This may help patients tolerate early dilator work, particularly when vestibular sensitivity is prominent.
Why Conventional Treatments Sometimes Fail
In severe vaginismus:
- Resting pelvic floor tone is markedly elevated
- Trigger points are present
- Guarding becomes reflexive
- Attempts at dilator insertion reinforce panic
In these cases, the muscle contraction is not simply behavioural — it is neurophysiologically embedded.
This is where Botox becomes a powerful adjunct.
Botox for Vaginismus: Mechanism of Action
Botulinum toxin type A (BoNT-A) is a neuromodulatory protein that acts at the neuromuscular junction.
Step 1: Blocking Acetylcholine Release
BoNT-A inhibits release of acetylcholine by cleaving SNAP-25 at the presynaptic terminal.
Without acetylcholine:
- Muscle fibres cannot contract
- Spasm reduces
- Resting tone decreases
This produces a temporary, reversible relaxation of the injected muscle lasting approximately 3–6 months.
Step 2: Reduction of Pain Mediators
In addition to motor effects, BoNT-A may:
- Reduce release of substance P
- Reduce peripheral sensitisation
- Modulate neurogenic inflammation
This is particularly relevant in patients with burning pain or features of pudendal neuralgia.
Step 3: Breaking the Reflex Arc
Vaginismus is sustained by a reflex arc:
Fear → Muscle contraction → Failed penetration → Reinforced fear.
By chemically reducing muscle contraction, Botox interrupts the mechanical component of this loop.
For the first time, penetration becomes physically possible without intense resistance.
This creates a therapeutic window.
What Does the Evidence Show?
Botox for vaginismus has been studied in treatment-resistant populations.
Meta-analysis Evidence
A systematic review and meta-analysis concluded that botulinum toxin is an effective therapeutic option for vaginismus, particularly in refractory cases, with a pooled odds ratio of 8.7.
However, authors emphasised the need for higher-quality randomized trials.
Systematic Review of Chronic Pelvic Pain
A broader review of botulinum toxin in chronic pelvic pain demonstrated improvement in pain scores in observational studies, with no serious adverse events reported.
Vulva and Vaginal BoNT Review
A 2023 systematic review found botulinum toxin improved:
- Vaginismus
- Dyspareunia
- Chronic pelvic pain
No irreversible complications were detected.
Dose Comparison Study
A comparative study of 150 vs 200 units demonstrated:
- Significant improvements in pain and anxiety
- No significant difference between doses
At Pain Spa, we typically commence treatment with 200 units of botulinum toxin, as this dose has been shown to be both safe and effective in clinical studies. Patients are reviewed at follow-up to assess response, functional progress, and the need for any further treatment in due course. Higher initial doses are not recommended, as the aim is to achieve the optimal balance between adequate muscle relaxation and preservation of functional pelvic floor control.
Important Context
While observational outcomes are encouraging, randomized trial data remains limited.
Therefore, Botox should be viewed as:
- A targeted intervention for selected patients
- Part of a structured multidisciplinary plan
- Not a standalone cure
Rehabilitation After Botox: The Critical Post-Treatment Phase
Botox is not a cure in isolation.
It reduces pelvic floor spasm, but it does not automatically retrain the nervous system, remove fear associations, or restore normal muscle coordination. The period following injection is therefore crucial.
Botox creates what we call a therapeutic window — typically lasting 3–6 months — during which:
- Muscle resistance is significantly reduced
- Penetration becomes mechanically possible
- Pain response is softened
- Anxiety often decreases
This is the optimal time to begin structured rehabilitation.
1. Graduated Dilator Therapy
After Botox, patients who previously could not tolerate even minimal insertion are often able to begin gentle dilation.
Dilator therapy now becomes:
- Less threatening
- Less painful
- More successful
The aim is not simply to “stretch” the vagina, but to:
- Re-train the brain–pelvic floor connection
- Replace fear with neutral or positive experiences
- Build confidence gradually
Without this step, muscle tone may gradually return once Botox wears off, as the fear-avoidance cycle remains intact.
2. Pelvic Floor Physiotherapy
Specialist pelvic physiotherapy enhances outcomes significantly.
Following Botox, physiotherapy focuses on:
- Down-training and Relaxation: Teaching the patient to recognise and release pelvic floor tension using diaphragmatic breathing and conscious muscle awareness.
- Reverse Kegels: Encouraging lengthening and expansion rather than contraction — particularly important in hypertonic pelvic floors.
- Myofascial Release: Addressing residual trigger points in the levator ani, bulbospongiosus, or obturator internus.
- Biofeedback (when appropriate): Helping patients visualise muscle relaxation and learn control over resting tone.
The goal is not permanent weakness — but restoration of normal, adaptable pelvic floor function.
3. Psychological and Nervous System Support
Vaginismus is strongly influenced by the fear–pain cycle. Even after muscle relaxation, the brain may still anticipate danger.
If anxiety, catastrophic thinking, or trauma-related hypervigilance remain unaddressed:
- The sympathetic nervous system remains activated
- Guarding can return
- Progress may stall
Psychological support helps:
- Break fear-avoidance patterns
- Reduce anticipatory anxiety
- Reframe pain expectations
- Support intimacy and relationship confidence
This is particularly important in long-standing cases.
Why This Phase Determines Long-Term Success
Botox interrupts the muscle spasm.
Rehabilitation rewires the system.
Without structured post-Botox therapy:
- Improvements may be temporary
- Muscle tone may gradually return
- Fear associations may persist
When Botox is combined with:
- Guided dilator progression
- Pelvic floor physiotherapy
- Psychological input where needed
Long-term outcomes are significantly more favourable with this approach. At Pain Spa, Botox is always considered part of a coordinated, multidisciplinary pathway — not a standalone intervention.
Seeking Help for Vaginismus
If you are experiencing symptoms of vaginismus and would like a comprehensive assessment, we encourage you to seek specialist support. At Pain Spa, we provide structured, multidisciplinary evaluation and tailored treatment plans designed to address pelvic floor hypertonicity, nervous system sensitisation, and the psychological components of the condition.
To arrange a consultation, please contact Pain Spa directly at clinic@painspa.co.uk or visit www.painspa.co.uk for further information.