Endometriosis and Persistent Pelvic Pain: A Mechanism-Based Approach to Treatment

Endometriosis and Persistent Pelvic Pain
Why pain can continue even after surgery — and what that means
Endometriosis is a chronic inflammatory condition affecting approximately one in ten women of reproductive age. For many women, hormonal therapy and surgical excision significantly improve symptoms. However, a substantial number continue to experience pelvic pain even after apparently successful treatment — and sometimes even when repeat MRI scans show no visible disease.
This situation can be deeply distressing.
Patients may be told their surgery was “successful” or that their scan is “normal,” yet their pain persists. This does not mean the pain is imagined. It does not mean surgery has failed. And it does not mean the symptoms are psychological.
Rather, it reflects the complex and multifactorial nature of pain in endometriosis.
The Role of Gynaecology: Treating the Disease First
It is important to be clear at the outset.
The definitive treatment of endometriosis itself is hormonal therapy and, where appropriate, surgical excision under the guidance of a specialist gynaecology team.
Hormonal therapies — including combined hormonal contraception, progestogens, dienogest, and GnRH analogues — aim to suppress oestrogen-driven inflammatory activity.
Surgical excision aims to remove visible endometriotic lesions, reduce inflammatory burden, and restore pelvic anatomy.
These interventions target the disease process.
Pain management interventions do not replace disease-directed therapy. Rather, they are considered in women whose pain persists despite appropriate hormonal and/or surgical management, or in those where additional pain mechanisms have become established.
At Pain Spa, we work alongside gynaecology colleagues. Our role is to assess and address the mechanisms that may remain active even after inflammatory disease has been treated.
Endometriosis Pain Is Multifactorial
Pain in endometriosis is rarely driven by a single mechanism. It often reflects overlapping contributors:
• Ongoing inflammatory nociceptive input
• Direct nerve involvement or irritation
• Post-surgical nerve sensitisation
• Myofascial pelvic floor dysfunction
• Abdominal wall trigger points
• Deep gluteal muscle involvement
• Visceral sensitisation
• Central sensitisation
Once these processes are established, pain may persist even after visible endometriosis has been removed.
Understanding these mechanisms is crucial in preventing repeated surgery when the primary drivers of pain are no longer inflammatory lesions, but neural, muscular, and central sensitisation processes.
Nerve Involvement in Endometriosis
Endometriosis can involve pelvic nerves directly, particularly in deep infiltrating disease.
Structures that may be affected include:
• Uterosacral ligaments
• Sacral plexus
• Pudendal nerve
• Sciatic nerve (rarely but significantly)
Inflammation, fibrosis, and scarring may also irritate somatic nerves such as:
• Ilioinguinal nerve
• Genitofemoral nerve
• Pudendal nerve
• Posterior femoral cutaneous nerve
• Inferior cluneal nerves
When nerves are irritated or infiltrated, pain may take on neuropathic characteristics including burning, electric shock sensations, radiating groin or buttock pain, perineal pain, sitting intolerance, and hypersensitivity.
Repeated inflammatory exposure can lead to peripheral sensitisation. In this state, the threshold for nerve activation is lowered, and amplified pain signals are transmitted even in response to minor stimuli.
Importantly, once a nerve becomes sensitised, pain may persist even if the original lesion has been removed. Post-surgical scarring may further contribute to mechanical irritation or tethering of nerves.
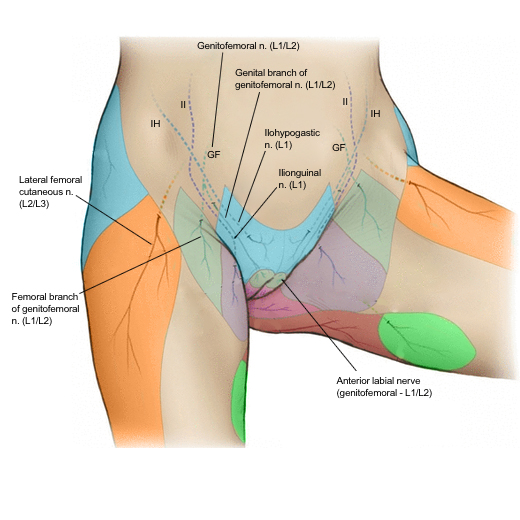
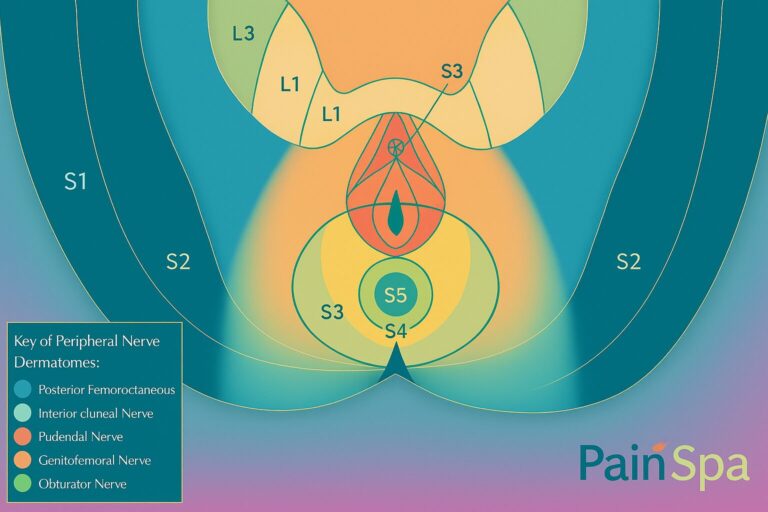
Peripheral Nerve Pain Distribution Maps
The following diagrams can be used in the blog to help patients understand why groin, perineal, buttock, or posterior thigh pain may reflect specific peripheral nerve territories rather than recurrent pelvic disease.
Myofascial Pain and Pelvic Floor Hypertonicity
Chronic pelvic pain frequently leads to protective muscle guarding. Over time, this guarding becomes maladaptive.
The pelvic floor is composed primarily of the levator ani complex, including pubococcygeus, puborectalis, and iliococcygeus. In addition, muscles such as obturator internus contribute to lateral pelvic wall support and functional integration with the pelvic floor.
Persistent contraction leads to reduced local blood flow, accumulation of metabolic by-products, development of trigger points, and sensitised muscle nociceptors. This transforms muscle into an independent pain generator.
Symptoms of pelvic floor hypertonicity may include deep pelvic aching, dyspareunia, rectal or vaginal pressure, sitting intolerance, pain with bowel movements, and hypersensitivity during examination.
Crucially, pelvic floor dysfunction does not appear on MRI and is not corrected by surgical excision. In many women with persistent post-surgical pain, pelvic floor hypertonicity becomes the dominant driver.
Anterior Abdominal Wall Trigger Points
Chronic pelvic pain often leads to co-contraction of the abdominal wall. Trigger points may develop in rectus abdominis, internal and external obliques, and transversus abdominis.
Symptoms may include localised abdominal tenderness, pain near surgical scars, hypersensitivity to light touch, and pain worsened by movement.
This may overlap with anterior cutaneous nerve entrapment syndromes, particularly after laparoscopy.
These muscular contributors do not appear on imaging, are not treated by pelvic surgery, and can perpetuate central sensitisation.
Piriformis and Obturator Internus
Deep buttock or groin pain may reflect muscular dysfunction rather than nerve damage.
Piriformis: spasm may cause deep gluteal pain, radiating discomfort, and sitting intolerance.
Obturator internus: dysfunction may cause deep pelvic pain, groin radiation, dyspareunia, and sitting intolerance, and it commonly coexists with pelvic floor hypertonicity.
These muscular contributors frequently persist despite removal of endometriotic lesions.
Visceral Sensitisation
Pelvic organs share converging neural pathways within the spinal cord.
Inflammation affecting one organ may increase sensitivity in adjacent organs. This phenomenon, known as visceral sensitisation, may explain:
• Bladder pain without infection
• IBS-type bowel symptoms
• Diffuse pelvic discomfort
Pain becomes more widespread because shared neural circuits become hyper-responsive.
Central Sensitisation: When the Nervous System Amplifies Pain
Pelvic organs share converging neural pathways within the spinal cord.
Inflammation affecting one organ may increase sensitivity in adjacent organs. This phenomenon, known as visceral sensitisation, may explain:
• Bladder pain without infection
• IBS-type bowel symptoms
• Diffuse pelvic discomfort
Pain becomes more widespread because shared neural circuits become hyper-responsive.
Why MRI Can Be Normal — Yet Pain Persists
MRI is excellent at detecting structural abnormalities such as:
• Endometriomas
• Deep infiltrating nodules
• Bowel or bladder involvement
However, MRI does not detect:
• Microscopic disease
• Nerve sensitisation
• Pelvic floor hypertonicity
• Trigger points
• Visceral hypersensitivity
• Central sensitisation
A normal MRI does not invalidate symptoms. It simply indicates that no large structural lesion is visible.
Persistent pain often reflects functional and neurobiological processes rather than recurrent disease.
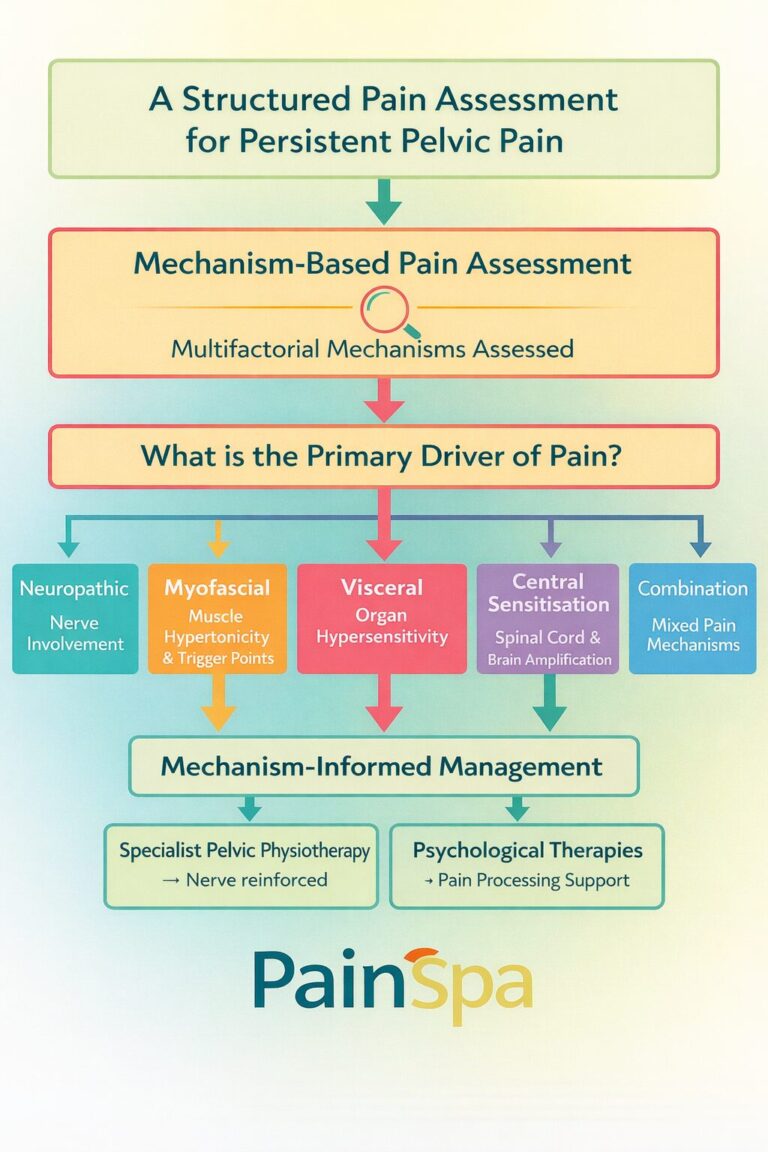
Mechanism-Based Pain Management Options
When dominant pain generators are identified, treatment can be directed accordingly. This approach moves away from repeated empirical or symptom-based treatments and instead targets the specific biological drivers maintaining pain.
It is important to emphasise that these interventions do not replace hormonal therapy or surgical management directed by the gynaecology team. Rather, they are considered in patients whose pain persists despite optimal disease treatment, or where additional neural and muscular mechanisms have become established.
A structured pain assessment aims to determine whether the primary driver is neuropathic, myofascial, visceral, centrally sensitised, or — as is often the case — a combination of these.
Treatment is therefore individualised, mechanism-informed, and delivered within a multidisciplinary framework.
The aim is not simply to “block pain,” but to reduce pathological amplification and restore functional tolerance.
Conservative Neuromodulatory Approaches
Before considering invasive interventions, conservative neuromodulatory strategies may be appropriate, particularly in patients with mixed nociceptive and central amplification components.
TENS (Transcutaneous Electrical Nerve Stimulation) may reduce pain through gate-control mechanisms at the spinal cord level and modulation of peripheral nociceptive input. By stimulating large-diameter afferent fibres, TENS can inhibit transmission of pain signals and may be particularly useful in managing flare-ups or cyclical exacerbations.
Acupuncture may influence pain modulation pathways, stimulate endogenous opioid release, and reduce sympathetic overactivity in selected patients. While evidence varies, some women with chronic pelvic pain report meaningful symptom reduction when acupuncture is incorporated into a broader rehabilitation strategy.
These approaches are not curative, but they may reduce overall pain burden, decrease reliance on medication, and improve tolerance to physiotherapy and functional rehabilitation.
Pelvic Health Physiotherapy
Specialist pelvic health physiotherapy is a cornerstone of management in women with persistent endometriosis-related pain.
When pelvic floor hypertonicity, myofascial dysfunction, or central sensitisation are present, rehabilitation becomes essential. Physiotherapy is not simply stretching exercises; it is a structured, mechanism-informed intervention.
Pelvic health physiotherapy may include:
• Down-training of overactive pelvic floor muscles
• Manual release of myofascial trigger points
• Breathing pattern retraining
• Desensitisation techniques
• Gradual exposure to previously painful movements
• Postural and biomechanical correction
• Functional rehabilitation
In patients with severe hypertonicity, physiotherapy may initially be poorly tolerated due to high baseline muscle tone. In such cases, interventions such as trigger point injections or botulinum toxin may be used to facilitate more effective rehabilitation.
Importantly, physiotherapy addresses the muscular and functional contributors to pain that are not visible on imaging and are not corrected by surgery.
For many patients, sustained improvement depends not on a single injection or procedure, but on progressive neuromuscular retraining delivered through specialist pelvic rehabilitation.
Trigger Point Injections
When significant myofascial dysfunction is identified, trigger point injections may be considered as part of a structured treatment plan.
Chronic muscle guarding leads to the development of hyperirritable nodules within taut bands of skeletal muscle. These trigger points are characterised by localised contracture, reduced perfusion, sensitised nociceptors, and abnormal motor endplate activity.
Trigger points may generate local pain, referred pain, and ongoing nociceptive input that perpetuates central sensitisation.
Targeted trigger point injections may be delivered to:
• Pelvic floor muscles (including levator ani components)
• Obturator internus
• Piriformis
• Rectus abdominis and other anterior abdominal wall muscles
In carefully selected patients, injections may reduce sustained muscle contraction, improve local circulation, decrease peripheral nociceptive signalling, interrupt the myofascial–central amplification cycle, and facilitate more effective engagement with pelvic physiotherapy.
In some cases, ultrasound guidance is used to enhance precision, particularly when targeting deeper muscles such as obturator internus or piriformis, where anatomical accuracy is important.
Trigger point therapy is not a standalone cure. Its role is to reduce amplification from myofascial sources and create a window of opportunity for neuromuscular retraining.
The Role of Botulinum Toxin in Pelvic Floor Hypertonicity
In selected patients with severe pelvic floor overactivity that has not responded adequately to specialist physiotherapy alone, botulinum toxin (Botox) may be considered.
Muscles commonly targeted may include levator ani (pubococcygeus, puborectalis, iliococcygeus), obturator internus, and deep perineal muscles (in selected cases). These muscles may remain in a state of sustained contraction long after the original inflammatory driver has settled.
The aim of treatment is not paralysis, but reduction of excessive resting tone.
Mechanism of action: botulinum toxin blocks acetylcholine release at the neuromuscular junction, thereby reducing excessive muscle contraction. Beyond mechanical relaxation, emerging evidence suggests additional effects including reduction of inflammatory neuropeptides, decreased peripheral nociceptive signalling, reduced spontaneous motor endplate activity, and indirect lowering of central amplification over time by reducing sustained nociceptive input.
Why Botox is combined with physiotherapy: severe hypertonicity may prevent effective manual therapy and down-training. Botox may reduce baseline muscle spasm, allow more effective stretching, facilitate desensitisation, improve tolerance to internal physiotherapy, and enable progressive neuromuscular retraining.
It does not treat endometriosis itself and does not replace gynaecological management. It is a targeted adjunct in appropriately selected patients.
Ultrasound-Guided Nerve Blocks
When neuropathic drivers are identified, image-guided nerve blocks may be considered as part of a mechanism-informed plan.
Target nerves may include:
- Ilioinguinal nerve
- Genitofemoral nerve
- Pudendal nerve
- Posterior femoral cutaneous nerve
- Inferior cluneal nerves
- Pain distribution patterns often correlate with these anatomical territories.
Ultrasound guidance allows direct visualisation of neural structures, identification of surrounding vessels, real-time needle placement, increased procedural precision, and reduced complication risk.
Nerve blocks may serve both diagnostic and therapeutic purposes. By temporarily reducing peripheral nociceptive input, they may help determine the dominant driver of pain and, in some cases, reduce peripheral sensitisation.
In selected patients, repeat treatments or adjunctive interventions may be considered depending on response and the broader rehabilitation plan.
Psychological and Pain Processing Support
Pain-focused psychological therapies aim to address central amplification, fear-avoidance, and maladaptive pain responses.
This does not imply the pain is psychological. It recognises that the nervous system can become sensitised and can be retrained, and that rehabilitation is more effective when the threat-response and protective behaviours around pain are addressed.
Psychological input is commonly integrated alongside physiotherapy and medical management within a multidisciplinary approach.
Frequently Asked Questions About Endometriosis and Persistent Pelvic Pain
Why do I still have pain after endometriosis surgery?
Persistent pain after surgery does not necessarily mean the operation failed. While surgery removes visible endometriotic lesions, it does not automatically reverse nerve sensitisation, pelvic floor muscle hypertonicity, or central pain amplification that may have developed over time.
In many women, these neural and muscular mechanisms continue to generate pain even after inflammatory disease has been addressed.
Can endometriosis pain persist even if my MRI scan is normal?
Yes. MRI scans detect structural abnormalities such as deep infiltrating lesions or endometriomas. However, MRI does not show nerve sensitisation, pelvic floor spasm, trigger points, visceral hypersensitivity, or central sensitisation.
A normal MRI does not invalidate symptoms. Persistent pain often reflects functional and neurobiological processes rather than recurrent visible disease.
Does persistent pain mean my endometriosis has come back?
Not necessarily. Recurrence of disease can occur in some patients, but persistent pain is frequently driven by neural or muscular mechanisms rather than new inflammatory lesions.
A structured assessment is important to distinguish between recurrent disease and sensitisation-based pain.
What is pelvic floor hypertonicity?
Pelvic floor hypertonicity refers to persistent overactivity and excessive resting tension in the pelvic floor muscles. These muscles may remain contracted due to long-standing pain or protective guarding.
This sustained contraction can itself become a source of pain and is not visible on imaging scans.
Can nerve involvement cause endometriosis pain?
Yes. Endometriosis may involve or irritate pelvic nerves, particularly in deep infiltrating disease. Even after surgery, sensitised nerves may continue to transmit amplified pain signals.
Symptoms such as burning pain, electric shock sensations, groin radiation, or sitting intolerance may suggest neuropathic involvement.
How can physiotherapy help endometriosis pain?
Specialist pelvic health physiotherapy addresses muscle overactivity, trigger points, breathing patterns, desensitisation, and neuromuscular retraining.
It targets the muscular and functional contributors to pain that are not corrected by surgery and is often central to long-term improvement.
When is botulinum toxin (Botox) considered?
Botulinum toxin may be considered in selected patients with severe pelvic floor hypertonicity that has not responded adequately to specialist physiotherapy.
It reduces excessive muscle contraction and may help facilitate more effective rehabilitation. It does not treat endometriosis itself but may address secondary muscular pain drivers.
Are nerve blocks a permanent solution?
Nerve blocks are not typically a permanent cure. They may serve diagnostic and therapeutic roles by reducing peripheral nociceptive input and helping identify the dominant pain generator.
They are usually incorporated into a broader mechanism-informed management plan.
Is persistent endometriosis pain psychological?
No. Persistent pain is a neurobiological process involving nerve sensitisation and central amplification. Psychological therapies may be helpful not because pain is imagined, but because the nervous system can become sensitised and can be retrained.
A multidisciplinary approach recognises both biological and nervous system contributions to pain.
Final Thoughts
Hormonal therapy and surgery remain the definitive treatments for endometriosis.
However, persistent pain may reflect neural, muscular, visceral, and central mechanisms that remain active after excision.
Persistent pain does not mean surgery failed. It does not mean MRI missed something. It does not mean symptoms are psychological.
It reflects the complexity of pain processing in endometriosis.
A structured, multidisciplinary approach can meaningfully improve quality of life in carefully selected patients.
If you are experiencing symptoms of endometriosis and would like a comprehensive assessment, we encourage you to seek specialist support. At Pain Spa, we provide structured, multidisciplinary evaluation and tailored treatment plans designed to address pelvic floor hypertonicity, nervous system sensitisation, and the psychological components of the condition.
To arrange a consultation, please contact Pain Spa directly at clinic@painspa.co.uk or visit www.painspa.co.uk for further information.