Gabapentin and Pregabalin for Nerve Pain: A Practical Guide to Effectiveness, Safety, and Tapering
Gabapentinoids in Pain Medicine: Benefits, Risks, and Why Long-Term Use Needs Careful Review
Understanding gabapentin and pregabalin in real-world pain practice
Introduction: Why This Conversation Matters Now
Gabapentinoids — gabapentin and pregabalin — were originally developed as antiepileptic medicines but are now widely prescribed in pain medicine, particularly for neuropathic pain. Over the past decade, prescribing increased substantially, partly driven by attempts to reduce opioid use.
However, off-label expansion into non-neuropathic pain conditions, long-term continuation without structured review, and emerging safety signals have prompted increasing scrutiny. Regulatory authorities have strengthened warnings regarding dependence, addiction, and withdrawal, and concerns have emerged regarding respiratory, cardiovascular, and possible cognitive risks.
Gabapentinoids can be effective for selected patients — but they are not benign, and they should never be prescribed indefinitely without active review.
What Are Gabapentinoids?
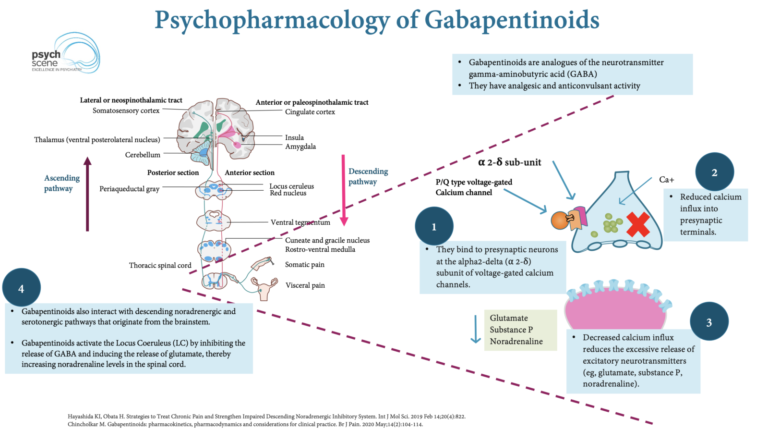
Gabapentin and pregabalin are structural analogues of gamma-aminobutyric acid (GABA). Despite this similarity, they do not act directly on GABA receptors.
They are licensed for:
- Neuropathic pain (e.g., post-herpetic neuralgia, diabetic neuropathy)
- Epilepsy (adjunct therapy)
- Pregabalin: fibromyalgia and generalised anxiety disorder (in some settings)
In clinical practice, they are frequently prescribed off-label for:
- Mechanical low back pain
- Sciatica
- Migraine
- Restless legs syndrome
- Peri-operative analgesia
In other words, these medicines were developed for nerve-based pain conditions but are often used far more broadly — sometimes without strong supporting evidence.
Structural and Molecular Differences Between Gabapentin & Pregabalin
Although both drugs are GABA analogues, they differ structurally.
Pregabalin is the S-enantiomer of 3-isobutyl GABA, whereas gabapentin contains a cyclohexane ring structure. These structural differences influence:
- Binding affinity to the α2δ-1 subunit of voltage-gated calcium channels
- Absorption characteristics
- Pharmacokinetic predictability
Pregabalin has a higher affinity for the α2δ-1 subunit and demonstrates more predictable absorption. This contributes to its often faster onset and perceived potency.
Neither drug is a prodrug.
In practical terms, pregabalin behaves more predictably pharmacokinetically — but this does not make it inherently safer.
Mechanism of Action
Gabapentinoids bind to the α2δ subunit of voltage-gated calcium channels, reducing presynaptic calcium influx and decreasing release of excitatory neurotransmitters including:
- Glutamate
- Noradrenaline
- Substance P
Put simply, they dampen overactive nerve signalling. This explains their usefulness in neuropathic pain — but they do not directly treat structural disc disease, muscle strain, or mechanical joint pathology.
Pharmacokinetics: Clinically Important Differences
Gabapentin and pregabalin differ meaningfully in absorption and bioavailability.
Gabapentin:
- Saturable absorption via L-amino acid transporters
- Oral bioavailability approximately 30–60%
- Non-linear kinetics
- Peak plasma concentration ~3 hours
Pregabalin:
- Rapid, near-complete absorption
- Bioavailability >90%
- Linear kinetics
- Peak plasma concentration ~1 hour
Clinically, increasing gabapentin dose does not proportionally increase plasma levels due to saturable transport. Pregabalin demonstrates more predictable dose-response behaviour.
Both drugs are renally excreted and require dose adjustment in renal impairment.
Evidence for Effectiveness
Neuropathic Pain
Moderate-quality evidence supports use in:
- Post-herpetic neuralgia
- Diabetic peripheral neuropathy
Comparative studies suggest pregabalin may provide faster symptom relief in certain neuropathic conditions, though both drugs can be effective when appropriately selected.
For clearly defined neuropathic pain, gabapentinoids remain reasonable therapeutic options.
Mechanical Low Back Pain and Sciatica
Evidence does not support routine use of gabapentinoids for mechanical low back pain, sciatica, or spinal stenosis. High-quality reviews conclude that, for most patients, these drugs do not perform better than placebo in non-neuropathic back pain and often produce more side effects than benefit.
This distinction is clinically critical.
Real-World Prescribing Patterns
Observational prescribing data demonstrate widespread use across musculoskeletal conditions, frequently at lower doses than recommended for neuropathic pain. This reflects expansion beyond the strongest evidence base.
Major Safety Concerns
Gabapentinoids and Cognitive Risk: Dementia and Mild Cognitive Impairment
Emerging observational studies have raised concerns about a possible association between long-term gabapentinoid use — particularly gabapentin — and dementia or mild cognitive impairment (MCI).
A large population-based cohort study using Taiwan’s National Health Insurance Research Database reported that exposure to gabapentin or pregabalin was associated with a significantly increased incidence of dementia (adjusted hazard ratio approximately 1.45), with stronger associations observed at higher cumulative doses and in younger patients.
More recently, a large U.S. retrospective cohort analysis published in Regional Anesthesia & Pain Medicine examined adults with chronic low back pain and found that patients receiving six or more gabapentin prescriptions had approximately 29% increased risk of dementia and approximately 85% increased risk of mild cognitive impairment, with the relative risk appearing even higher in adults aged 18–64.
These studies are observational and do not prove causation. Chronic pain itself, comorbidities, lifestyle factors, and polypharmacy may contribute. However, the consistency of the signal across large datasets suggests that prolonged gabapentinoid exposure should not be considered entirely benign.
Clinical implication: Patients on long-term gabapentinoids should be regularly reviewed for cognitive symptoms, and ongoing treatment should be justified by meaningful benefit — particularly in younger or middle-aged adults.
Gabapentinoids Co-Prescribed with Opioids: Respiratory and Mortality Risk
The combination of gabapentinoids and opioids has been repeatedly associated with increased risk of serious harm.
A landmark population-based study (Gomes et al., PLoS Medicine, 2017) demonstrated that concomitant gabapentin use in patients prescribed opioids was associated with approximately 50% increased risk of opioid-related death, with higher gabapentin doses conferring even greater risk.
Subsequent inpatient case-control analyses have shown that co-administration of gabapentinoids and opioids is associated with significantly increased odds of opioid-related overdose.
Mechanistically, gabapentinoids may:
- Potentiate central nervous system depression
- Reverse opioid tolerance to respiratory suppression
- Produce additive respiratory depressant effects
Regulatory agencies, including the FDA and MHRA, have issued warnings about serious breathing difficulties when gabapentinoids are combined with opioids or other sedatives.
Patients at particular risk include those with:
- COPD
- Sleep apnoea
- Advanced age
- Polypharmacy
- High opioid doses
Clinical implication: Gabapentinoid-opioid combinations should be avoided where possible. If clinically justified, they require careful risk assessment, lowest effective dosing, and close monitoring.
Misuse, Dependence, and Diversion
Systematic reviews confirm that both gabapentin and pregabalin have misuse potential. Pregabalin appears to carry a stronger misuse signal in some datasets, particularly among individuals with psychiatric or substance use histories.
Gabapentinoids are now controlled drugs in the UK due to rising misuse and associated fatalities.
Withdrawal and Abrupt Discontinuation
Abrupt cessation can result in:
- Anxiety
- Insomnia
- Agitation
- Sweating
- Tachycardia
- In rare cases, severe psychiatric disturbance
Case reports describe depression with psychotic features following sudden pregabalin discontinuation.
Gradual tapering is essential.
Cardiovascular and Thromboembolic Signals
A recent systematic review analysing over one million patients reported associations between chronic gabapentinoid use and:
- Increased myocardial infarction risk after one year
- Increased stroke risk after five years
- Increased deep vein thrombosis and pulmonary embolism risk
These findings are observational and do not establish causality but reinforce the need for risk-benefit assessment in long-term therapy.
Dosing Principles: Start Low, Go Slow
- Initiate at low dose
- Titrate gradually
- Adjust for renal function
- Set expectations clearly
Dose changes should occur over weeks rather than days, with predefined review points.
At initiation, it is good practice to agree what constitutes meaningful benefit, how long the trial will last, and what the tapering plan would be if ineffective.
Review and Deprescribing
Gabapentinoids should be reviewed within 3–6 months of initiation.
Key questions include:
- Is pain meaningfully improved?
- Are side effects present?
- Is the original indication still valid?
- Are we treating neuropathic pain — or something else?
If benefit is unclear, gradual dose reduction should be considered.
Patients should never stop suddenly without medical advice.
Choosing Between Gabapentin and Pregabalin
The decision is not simply “which is stronger.” It depends on:
- Renal function
- Previous response
- Risk of misuse
- Side-effect profile
- Cost and formulary
- Need for predictable kinetics
Pregabalin offers more predictable absorption but may carry stronger misuse signals in some populations. Gabapentin may be preferable in selected higher-risk individuals, though absorption is less predictable.
Treatment should be individualised.
Comparative Summary Table: Gabapentin vs Pregabalin
| Feature | Gabapentin | Pregabalin |
|---|---|---|
| Absorption | Saturable transport (dose increases may not proportionally increase levels) | More complete, predictable absorption |
| Bioavailability | ~30–60% (variable) | >90% (more consistent) |
| Kinetics | Non-linear | Linear |
| Time to peak | ~3 hours | ~1 hour |
| Evidence base | Neuropathic pain benefit in selected cases; limited in mechanical pain | Neuropathic pain benefit in selected cases; limited in mechanical pain |
| Misuse signal | Present | Often stronger signal in some datasets |
| Key practical point | Less predictable at higher doses due to saturable absorption | More predictable titration, but predictability does not equal safety |
Pain Spa Perspective: Mechanism-Based, Not Reflex Prescribing
At Pain Spa, gabapentinoids are not prescribed or continued simply because pain exists.
We:
- Confirm neuropathic features and a plausible mechanism
- Explain realistic benefits and limitations
- Screen for respiratory, psychiatric, cardiovascular, and misuse risk
- Use the lowest effective dose
- Plan structured review
Where a clear peripheral pain generator exists, targeted image-guided interventions may be considered as part of a broader strategy.
Where central sensitisation or widespread persistent pain dominates, education, physiotherapy, sleep optimisation, and psychological strategies are prioritised over escalating medication or procedures.
The goal is rational, individualised, and safe care.
Conclusion
Gabapentinoids remain useful for selected neuropathic pain conditions. However, emerging evidence highlights limited benefit in non-neuropathic pain, increased risk when combined with opioids, misuse potential, withdrawal risk, and observational signals regarding cardiovascular and cognitive outcomes.
They should be prescribed thoughtfully, reviewed regularly, and reduced when benefit no longer clearly outweighs risk.
If you are taking gabapentin or pregabalin and are unsure whether it is still helping, it is entirely reasonable to request a medication review.
At Pain Spa, we are happy to work with you and your GP to assess whether gabapentinoids remain appropriate or whether alternative strategies may better support your pain and overall health.
Frequently Asked Questions (FAQ)
Are gabapentin and pregabalin the same thing?
No. They are in the same drug family (gabapentinoids) and work in similar ways, but they differ in how they are absorbed and how predictable their effects are. Pregabalin is usually absorbed more reliably, while gabapentin absorption can become saturated at higher doses.
What types of pain do gabapentinoids help the most?
They are most helpful for clearly defined neuropathic pain (nerve pain), such as post-herpetic neuralgia and diabetic neuropathy, when used thoughtfully and reviewed regularly.
Do gabapentinoids help mechanical back pain or sciatica?
For most people with mechanical low back pain, sciatica, or spinal stenosis, gabapentinoids do not perform better than placebo and can cause side effects. They should not be used routinely in these conditions unless there are clear neuropathic features and a strong rationale.
Why is it risky to combine gabapentinoids with opioids?
When combined with opioids, gabapentinoids can increase sedation and suppress breathing, raising the risk of overdose or serious respiratory complications. The risk is higher in people with COPD, sleep apnoea, older age, or multiple sedating medicines.
Can gabapentin or pregabalin cause dependence or withdrawal?
Yes. Some patients can develop dependence, and stopping suddenly can cause withdrawal symptoms such as anxiety, insomnia, agitation, and in rare cases severe psychiatric symptoms. If the medicine is no longer helping, it should usually be reduced gradually rather than stopped abruptly.
Is there evidence that gabapentinoids are linked to dementia?
Some large observational studies have reported an association between longer-term gabapentinoid use (particularly gabapentin) and higher rates of dementia or mild cognitive impairment. These studies do not prove causation, but they reinforce the importance of regular review and avoiding indefinite prescribing without clear benefit.
How often should gabapentinoids be reviewed?
A sensible approach is to review within 3–6 months of starting, and regularly thereafter. The key question is whether the medicine is delivering meaningful benefit that outweighs risks and side effects.
What does Pain Spa do differently?
At Pain Spa, we focus on mechanism-based assessment and avoid “reflex prescribing.” We identify whether pain is neuropathic, screen for medication risks, and use the lowest effective dose with a structured plan for review. Where appropriate, we may consider image-guided injections as part of a broader plan, but we also recognise that procedures are not right for everyone, especially when central sensitisation is the dominant driver.
If I’m taking gabapentin or pregabalin and I’m unsure it helps, what should I do?
It is reasonable to request a medication review. Never stop suddenly without medical advice. If benefit is unclear, a gradual, supported reduction is often safer and more comfortable.